Medullary carcinoma
Medullary thyroid carcinoma (MTC) accounts for about 5% of thyroid cancers. Differently from the other carcinomas, which arise from the follicular cells, medullary carcinoma arises from parafollicular cells (C cells) of the thyroid, which synthetize calcitonin. About 80-90% are sporadic and occur in adults, the rest occur in children in genetic syndromes called multiple endocrine neoplasia (MEN). Patients with MEN 2a (Sipple`s syndrome) develop this neoplasm together with pheochromocytoma and sometimes with a hyperplasia or an adenoma of the parathyroid. Patients with MEN 2b (mucosal neuroma syndrome) have medullary carcinoma, pheochromocytoma, multiple mucosal neuromas and a marfanoid habitus. About 90% of this tumors secrete calcitonin and the patient`s serum can be used to screen for them.
Cytologic diagnostic features
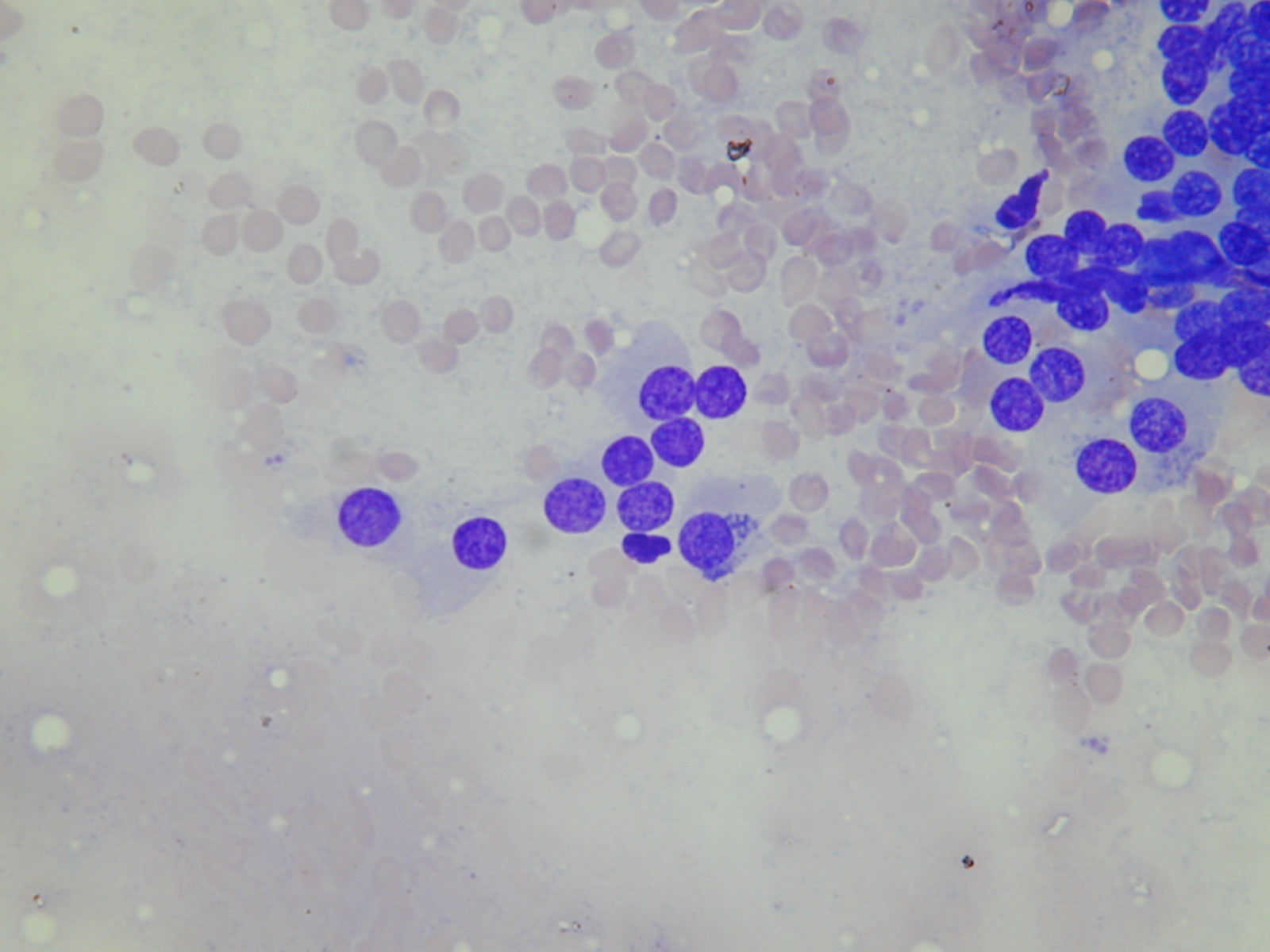
- mostly single cells
- loose clusters, trabeculae, rosettes
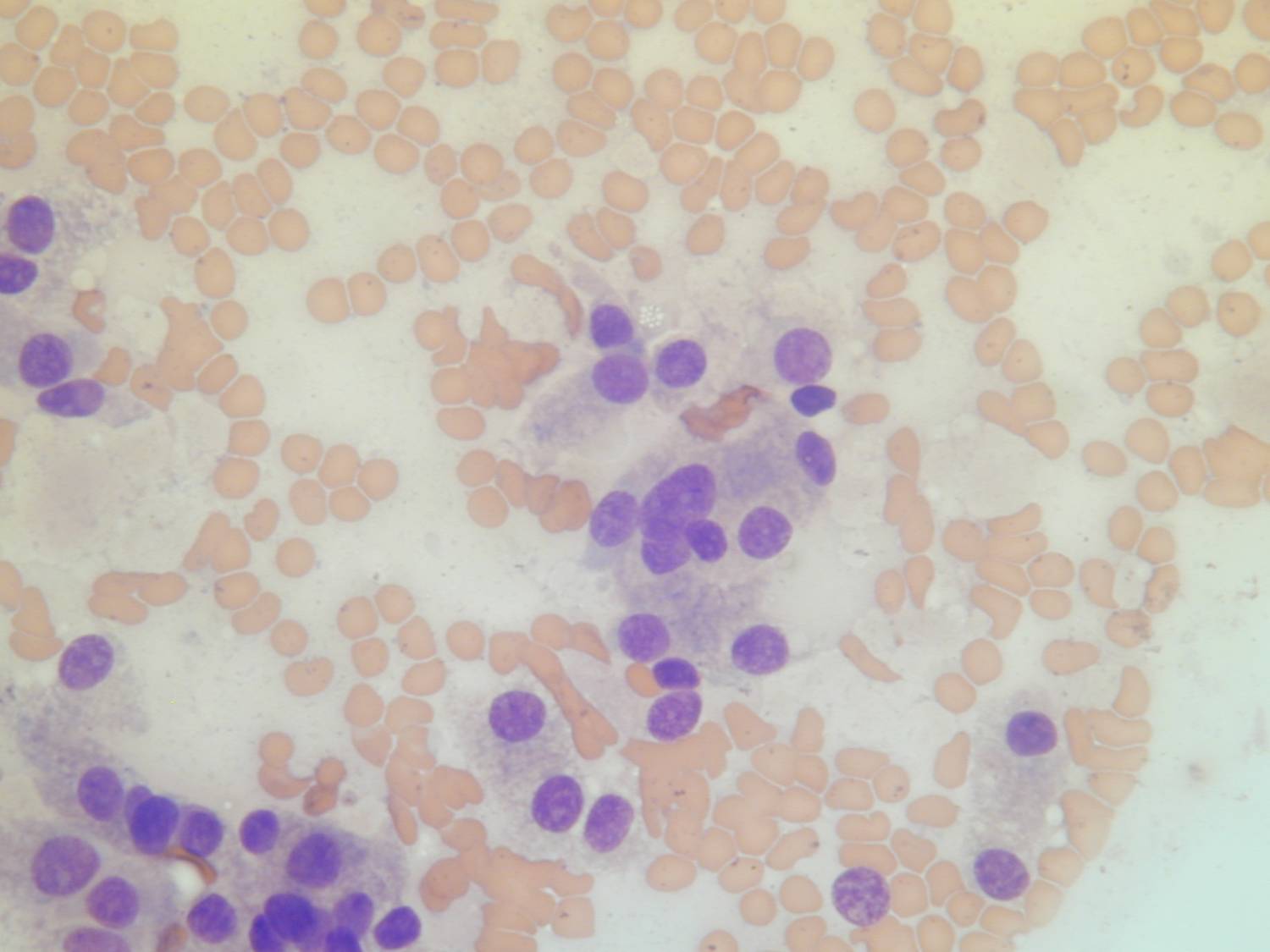
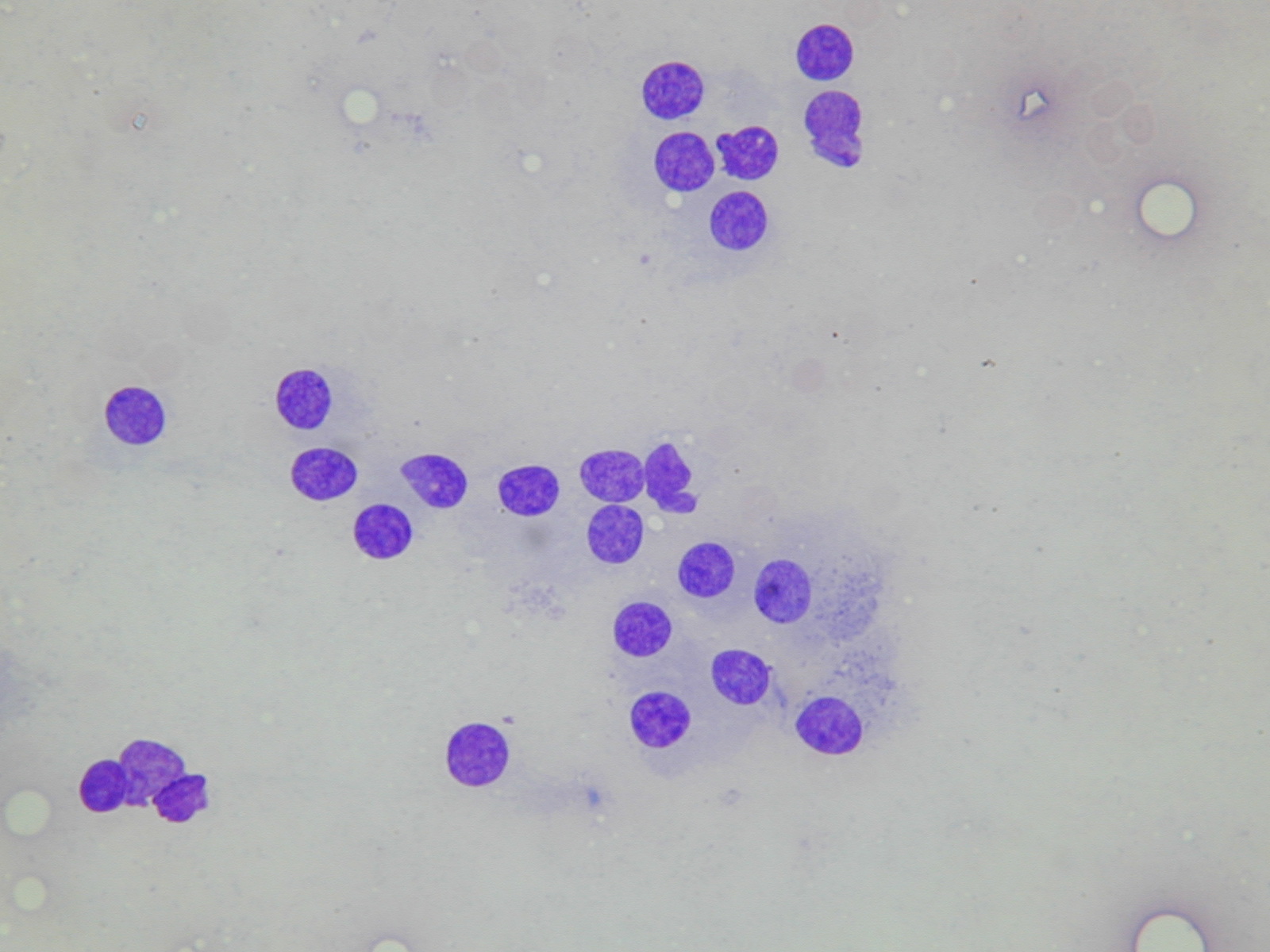
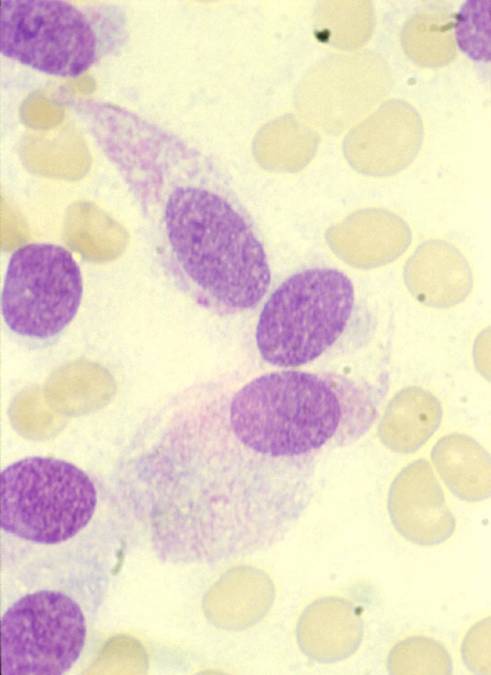
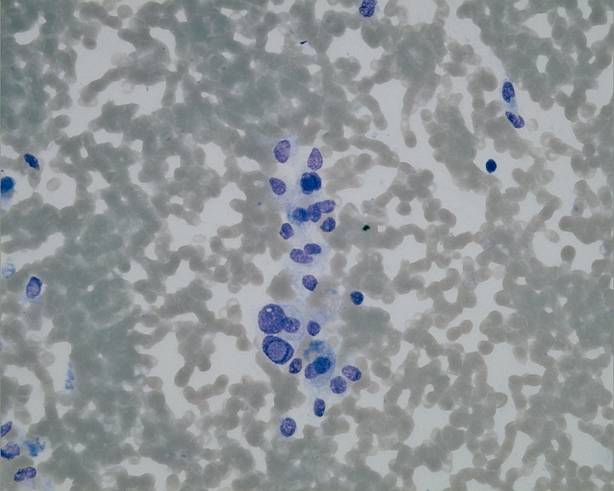
- plasmacytoid, epithelioid and/or spindle-shaped cells
- round nuclei, with 'salt and pepper' or coarsely granular chromatin
- cytoplasmic granules
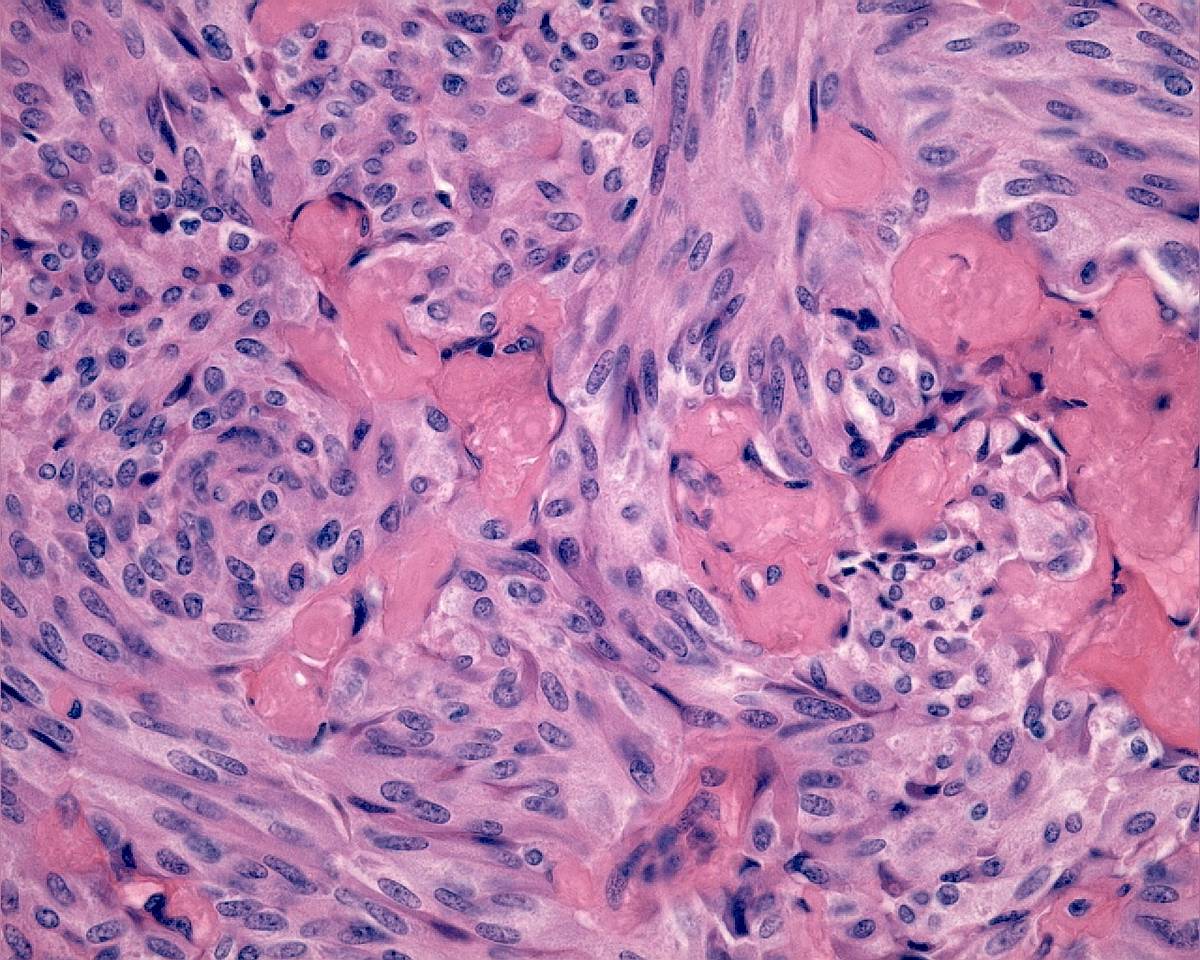
- amyloid
The cytologic pattern is variable. The cells are usually uniform in size and shape, but in many cases some very large cells may be observed. Most cells have fairly abundant basophilic cytoplasm, which typically may contain tiny neurosecretory granules that are red with Romanowski-type stains and metachromatic on May-Grünwald-Giemsa. The cytoplasm may be eccentric, imparting a 'plasmacytoid' appearance, or elongated. Some cells may be binucleated or multinucleated. Amyloid is present in some cases. It is similar to colloid, but it often contains stretched and distorted fibroblast nuclei. Its presence can be confirmed by a Congo red stain.
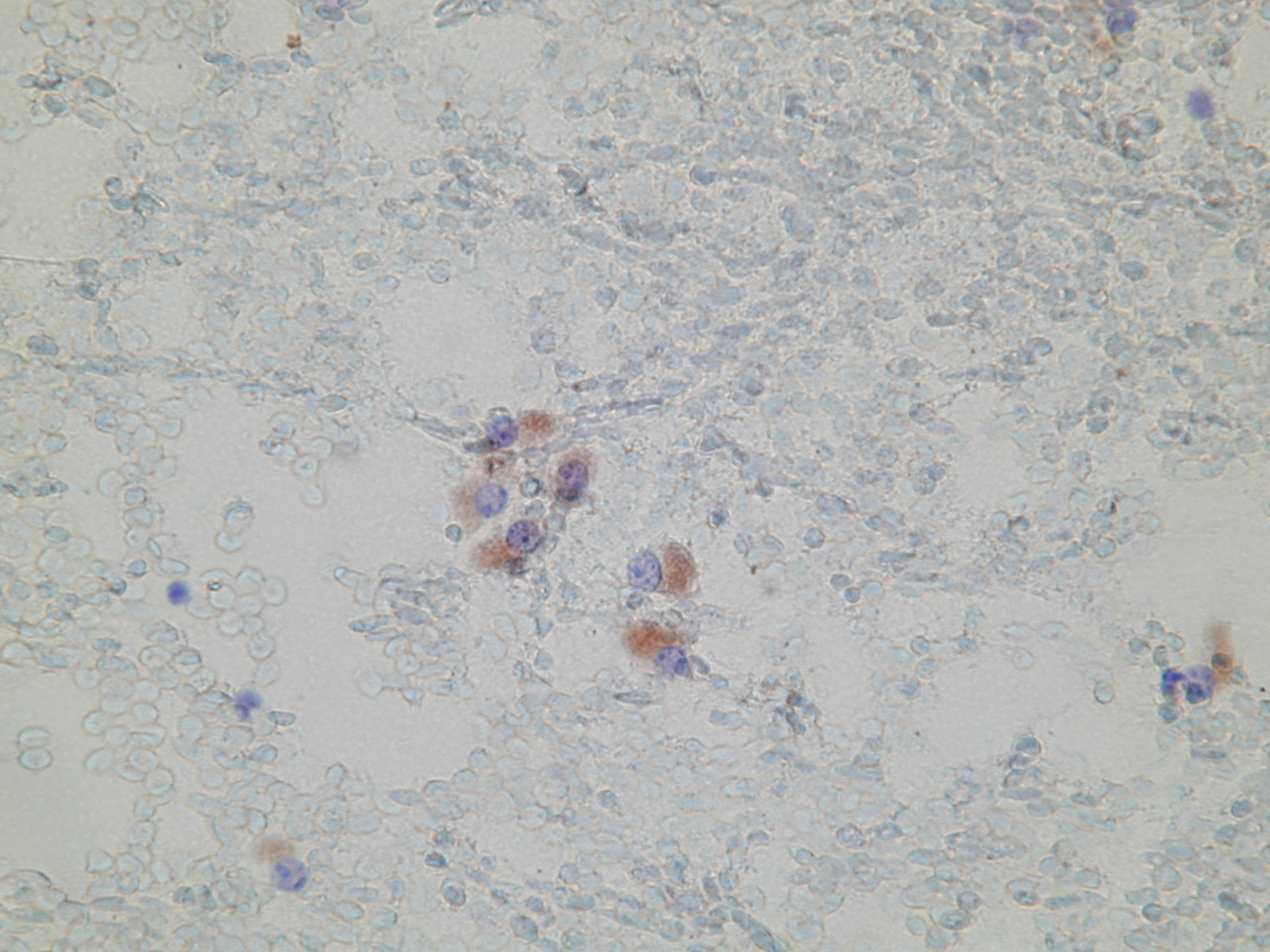
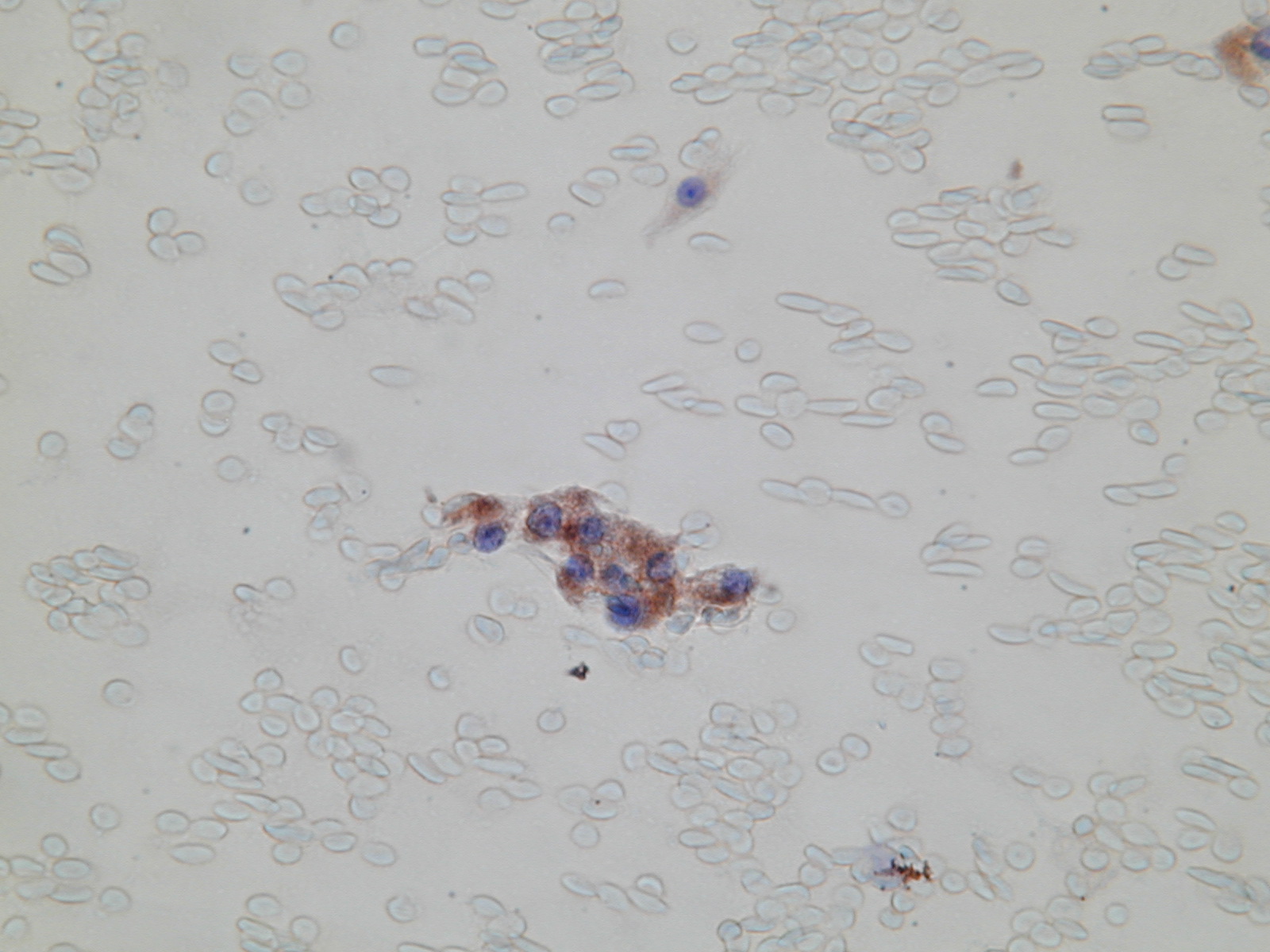
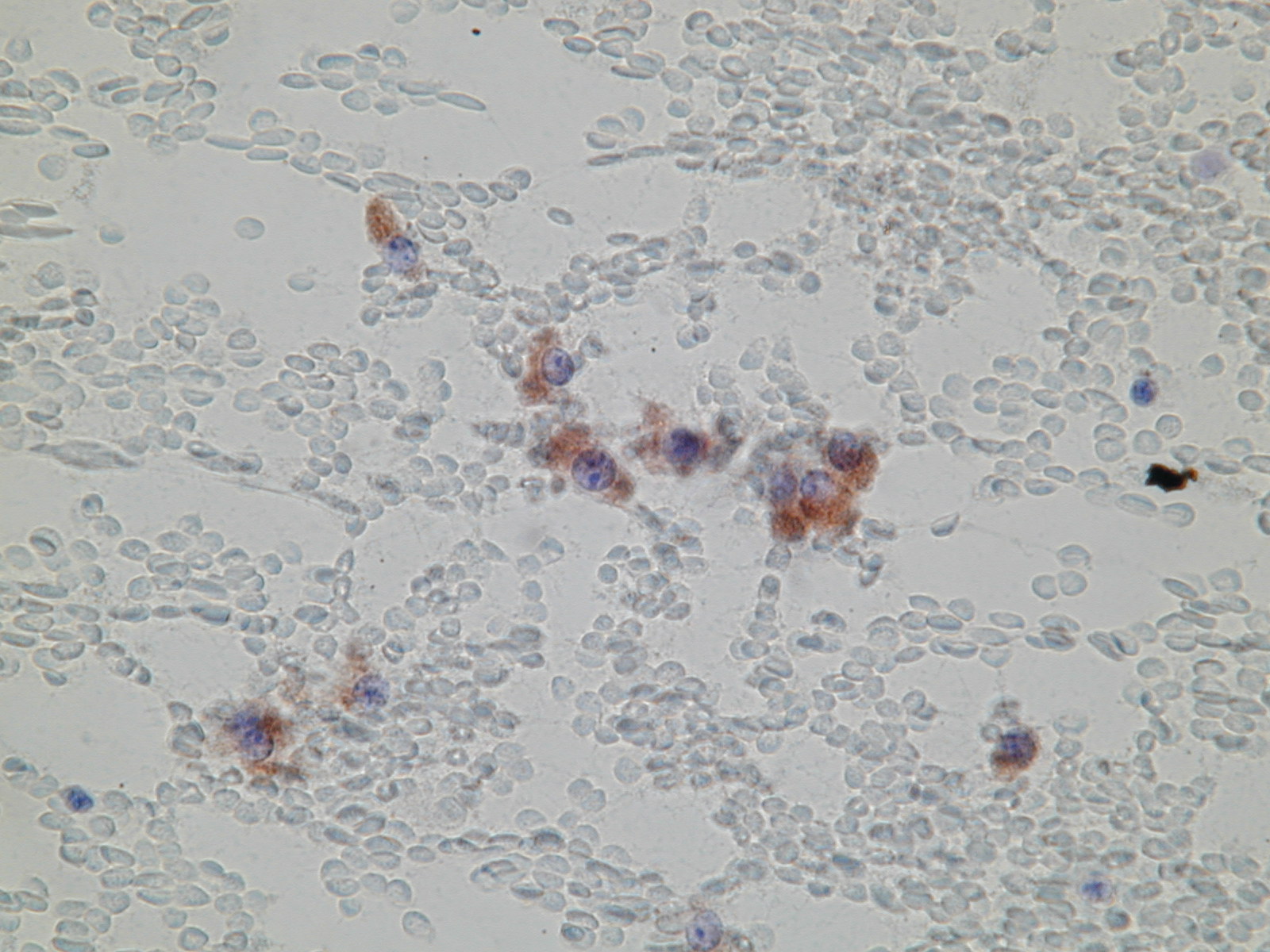
The neoplastic cells show positive immunocytochemical staining for calcitonin and for carcinoembyonic antigen (CEA).Differential diagnosis
- anaplastic carcinoma
- metastatic tumor
- Hürthle cell tumor
- follicular neoplasm
- insular carcinoma
- papillary carcinoma
Prominent nucleoli, like in Hürthle cell tumors, are not seen in medullary carcinoma, which has more hyperchromatic nuclei with coarsely granular chromatin. Medullary carcinoma can have spindle cells, but not giant cells and marked nuclear atypia like in anaplastic carcinoma. In doubt cases, positive immunocytochemical staining for calcitonin or an elevated serum calcitonin level is helpful to confirm the diagnosis.
Most of medullary carcinomas are correctly diagnosed by FNA; about 25% are misdiagnosed as other neoplasms.
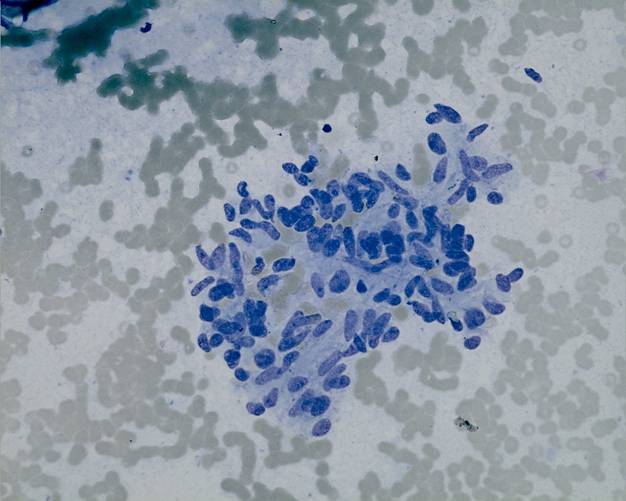
Discohesive elongated and 'plasmacytoid' cells (Pap). The nuclei have a coarsely granular chromatin and nucleoli are incospicuous (Pap). Discohesive tumour cells with dense, granular cytoplasm (MGG).
Typical appearance of neuroendocrine granules on MGG. A calcitonin stain on archival FNA material.
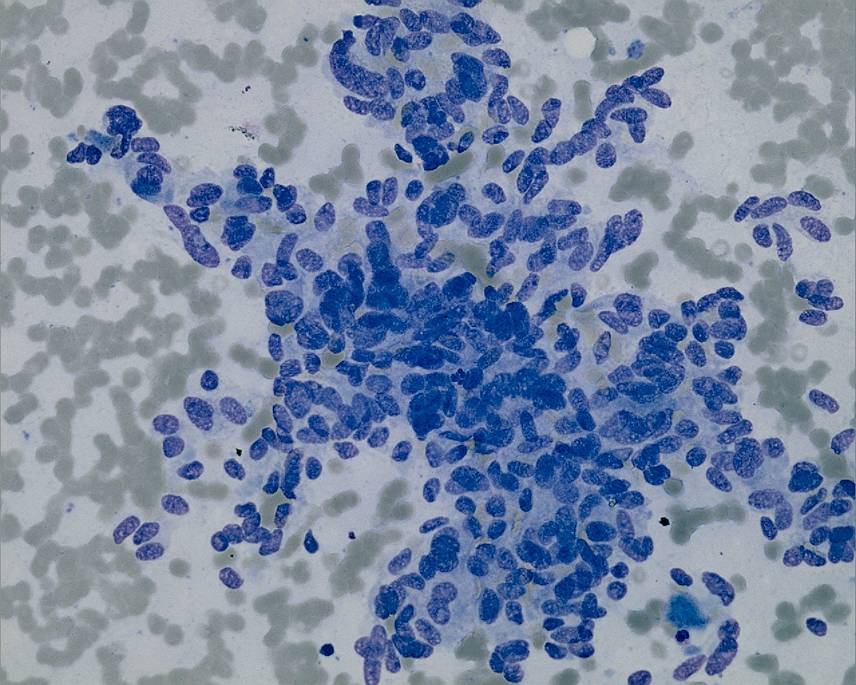
Discohesive "plasmacytoid" cells with dense cytoplasm and typical chromatin pattern (MGG). Cells from a MTC mimicking oncocytic changes (Pap). At higher power the typical chromatin pattern is apparent (Pap).
Calcitonin positive cells. Nuclear pseudoinclusions may be seen (MGG). A cluster of atypical spindle cells (MGG).
A large fragment of elongated atypical cells (MGG). A histological section from the same tumour (H&E).