

| Physiopathology of the effusions |
| Specimen collection and preparation methods |
| Accuracy |
| Reporting terminology |
| Benign elements |
| Non-neoplastic conditions |
| Malignant effusions |
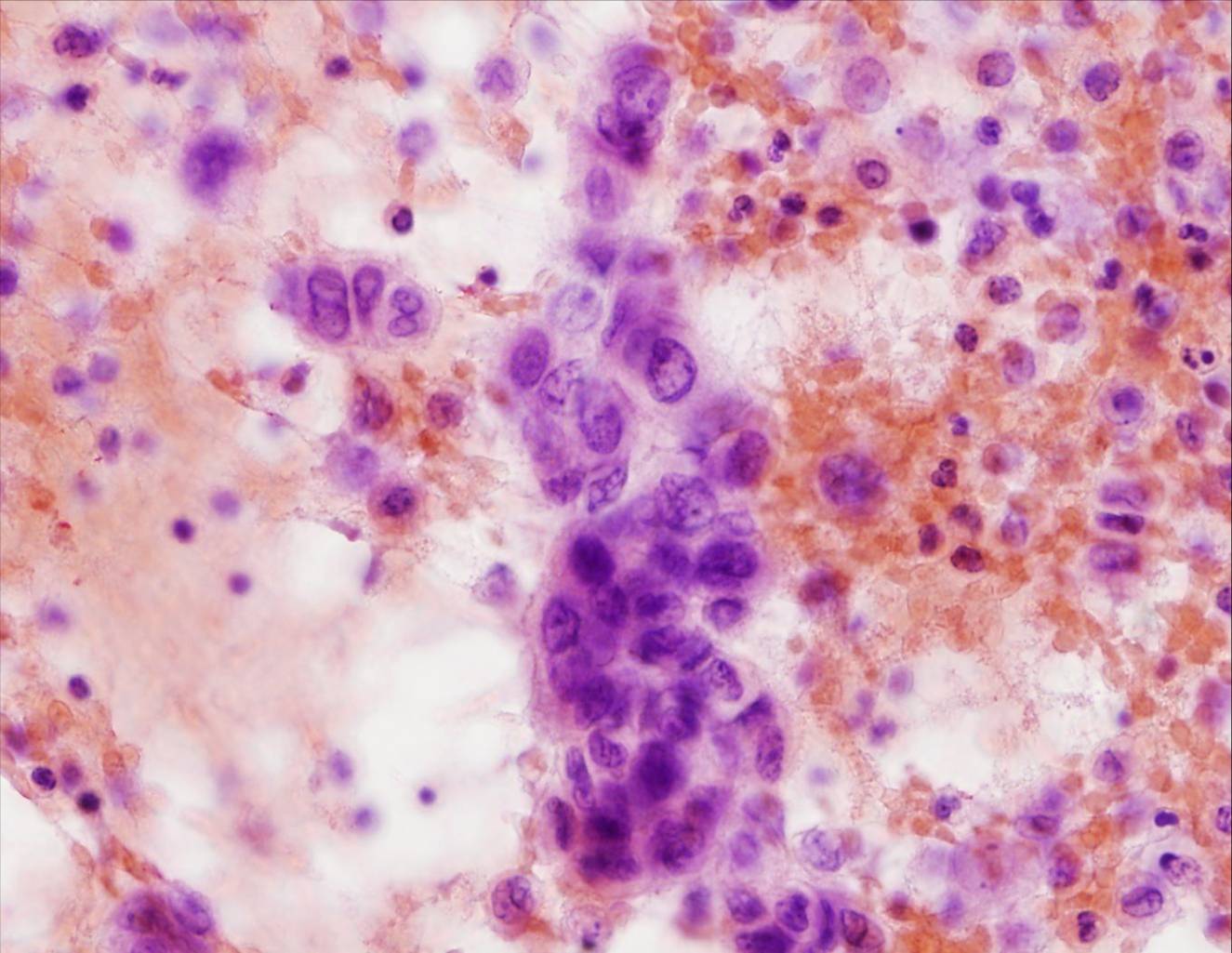
Metastatic carcinoma
Metastatic carcinomas are by far the most common tumors found in effusions. Adenocarcinomas are more common than squamous cell or undifferentiated carcinomas.
Histologic types which can be diagnosed:
- Adenocarcinoma
- Small cell carcinoma
- Squamous cell carcinoma
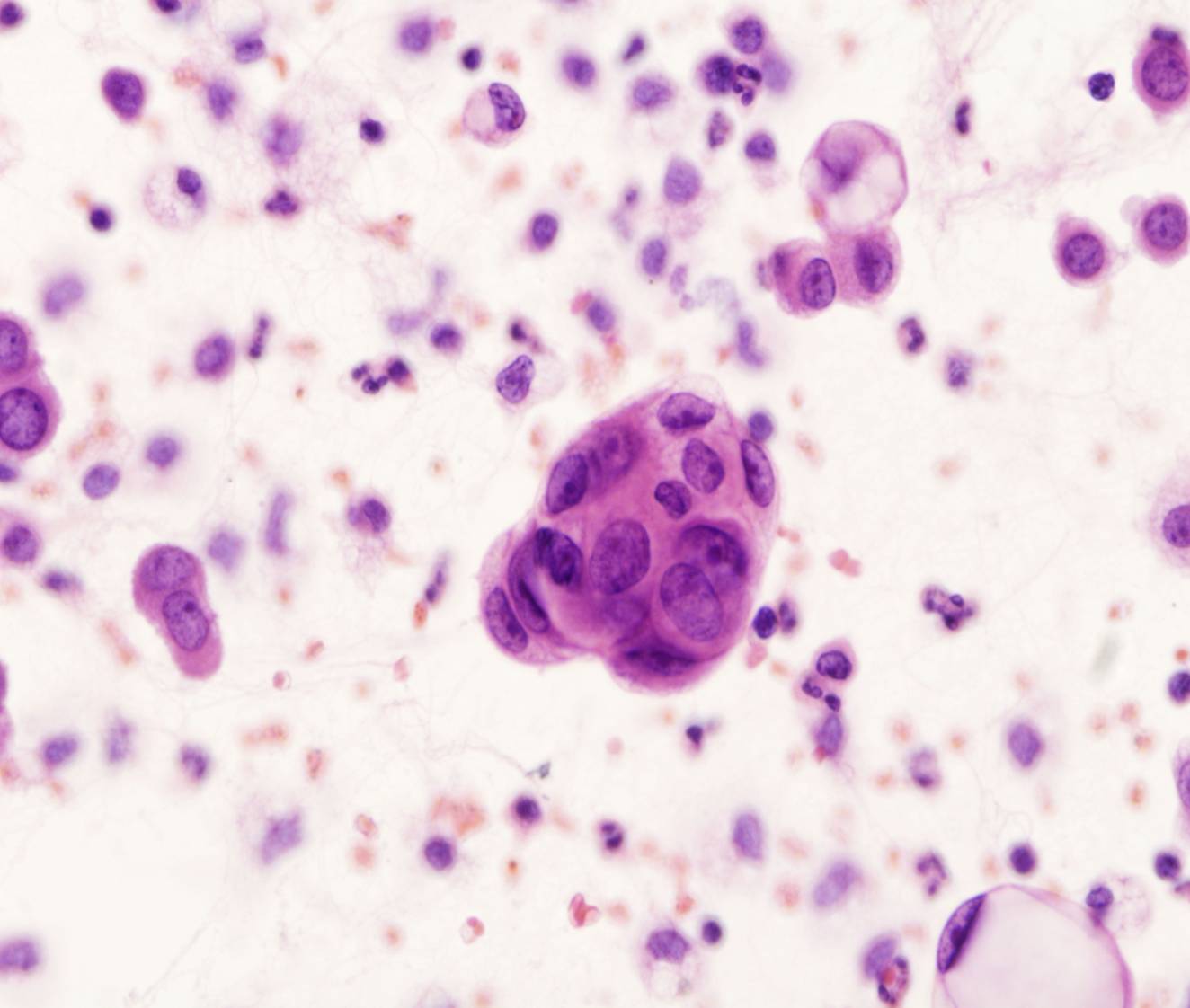
In most cases the cells are morphologically distinct from mesothelial cells. They are often larger and more pleomorphic than mesothelial cells, but they can be smaller and more uniform in size as well. Most commonly, they are distinguished from mesothelial cells by their tendency to form large clusters; however, some carcinomas exfoliate as isolated cells.
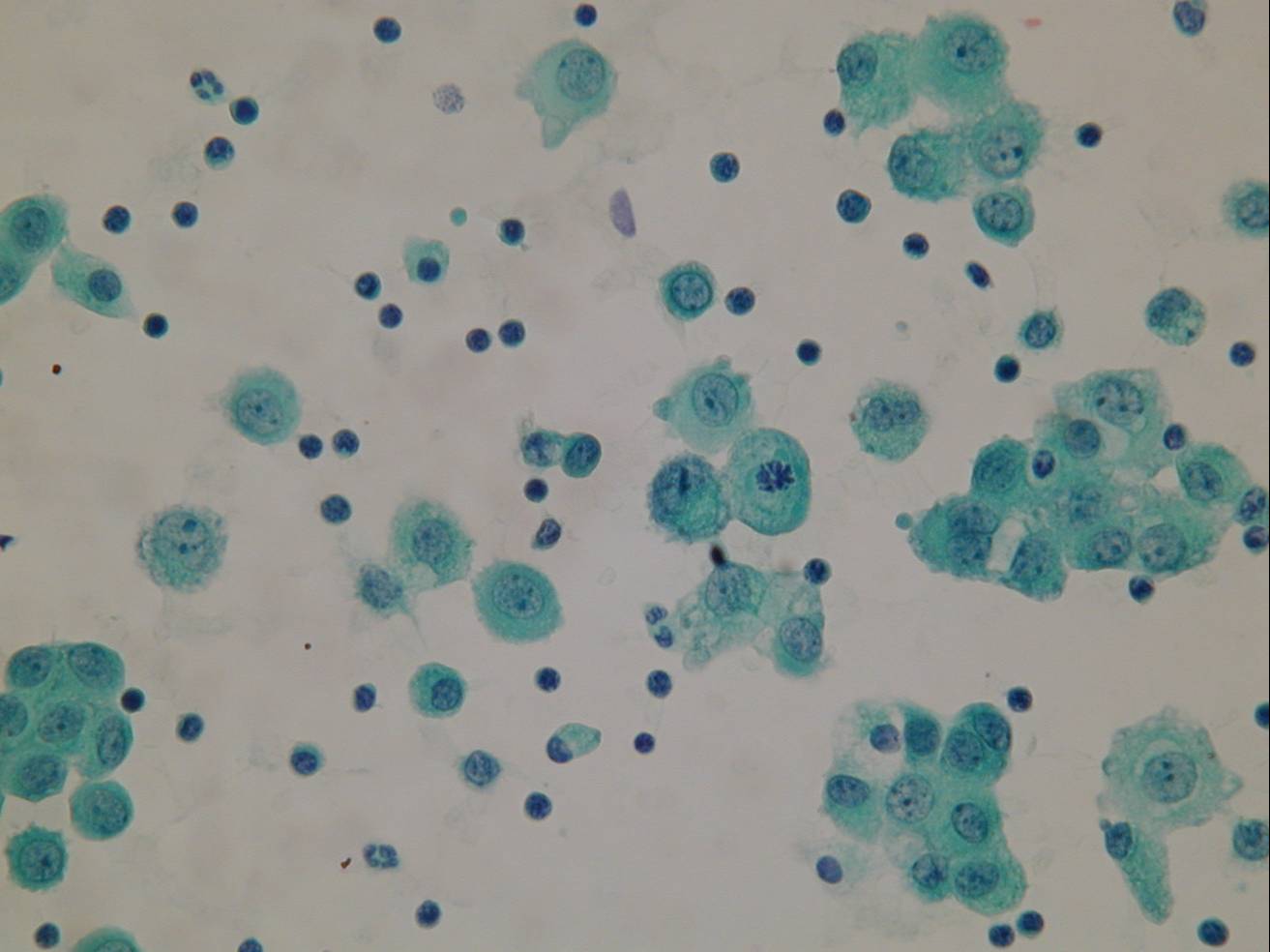
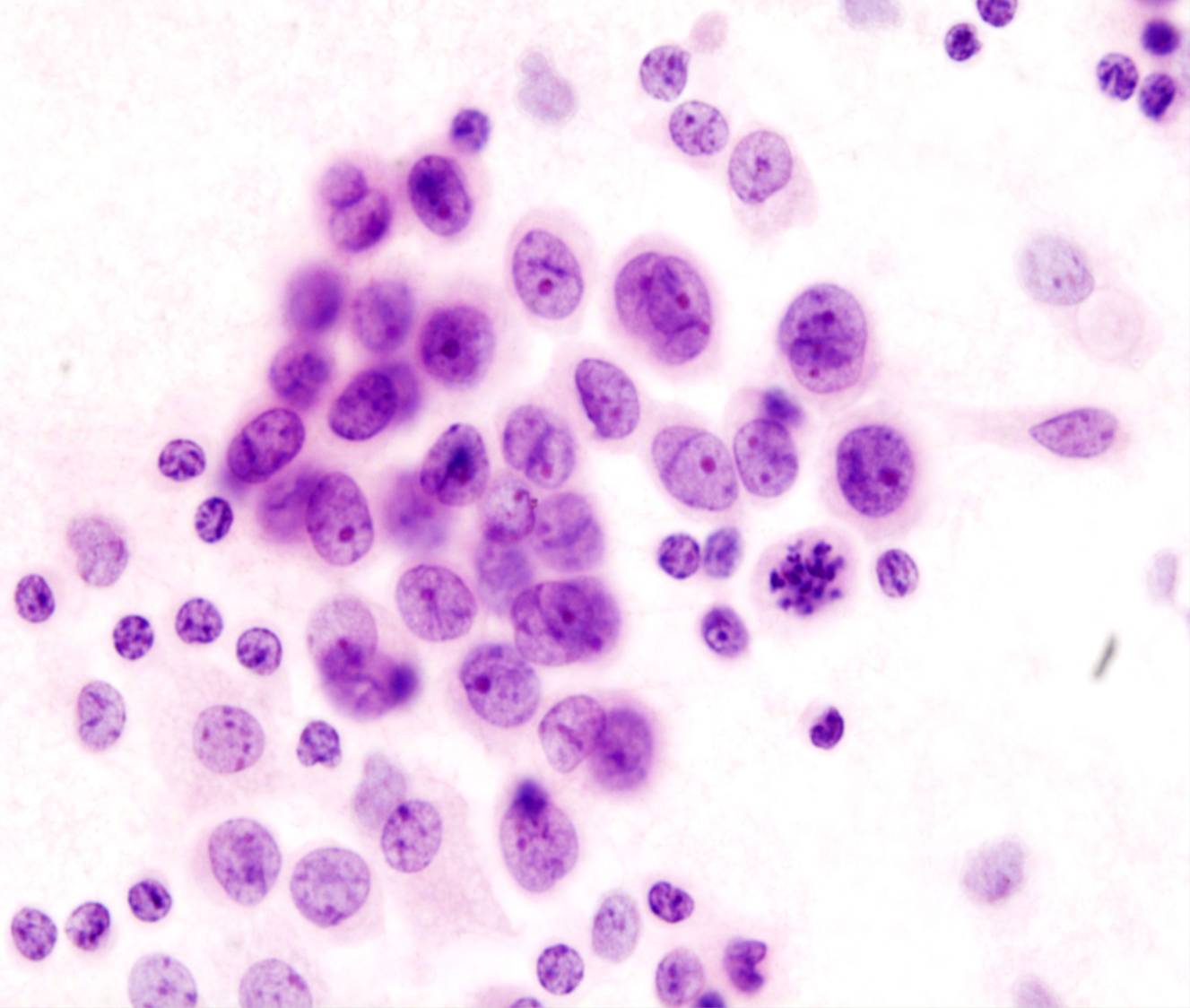
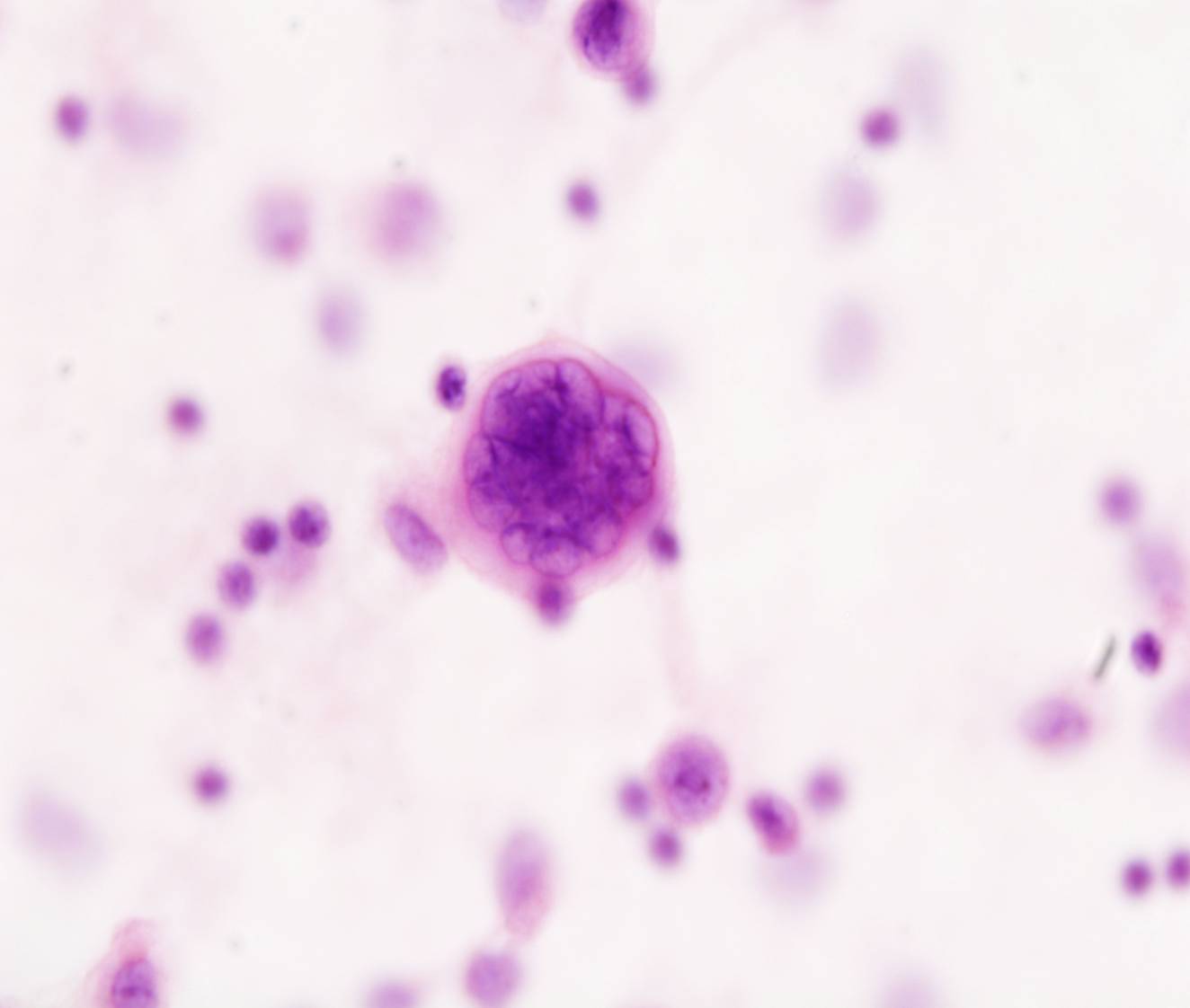
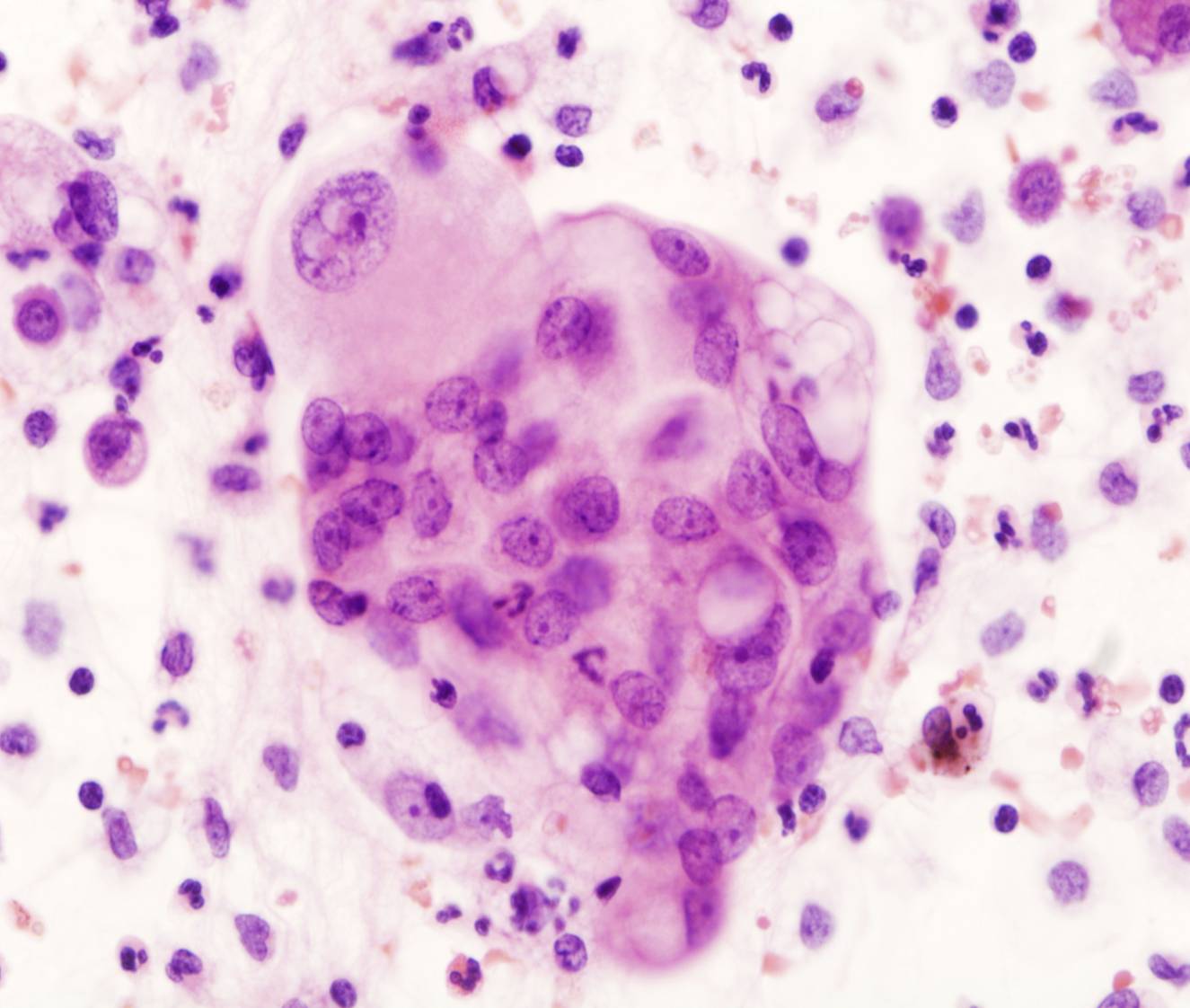
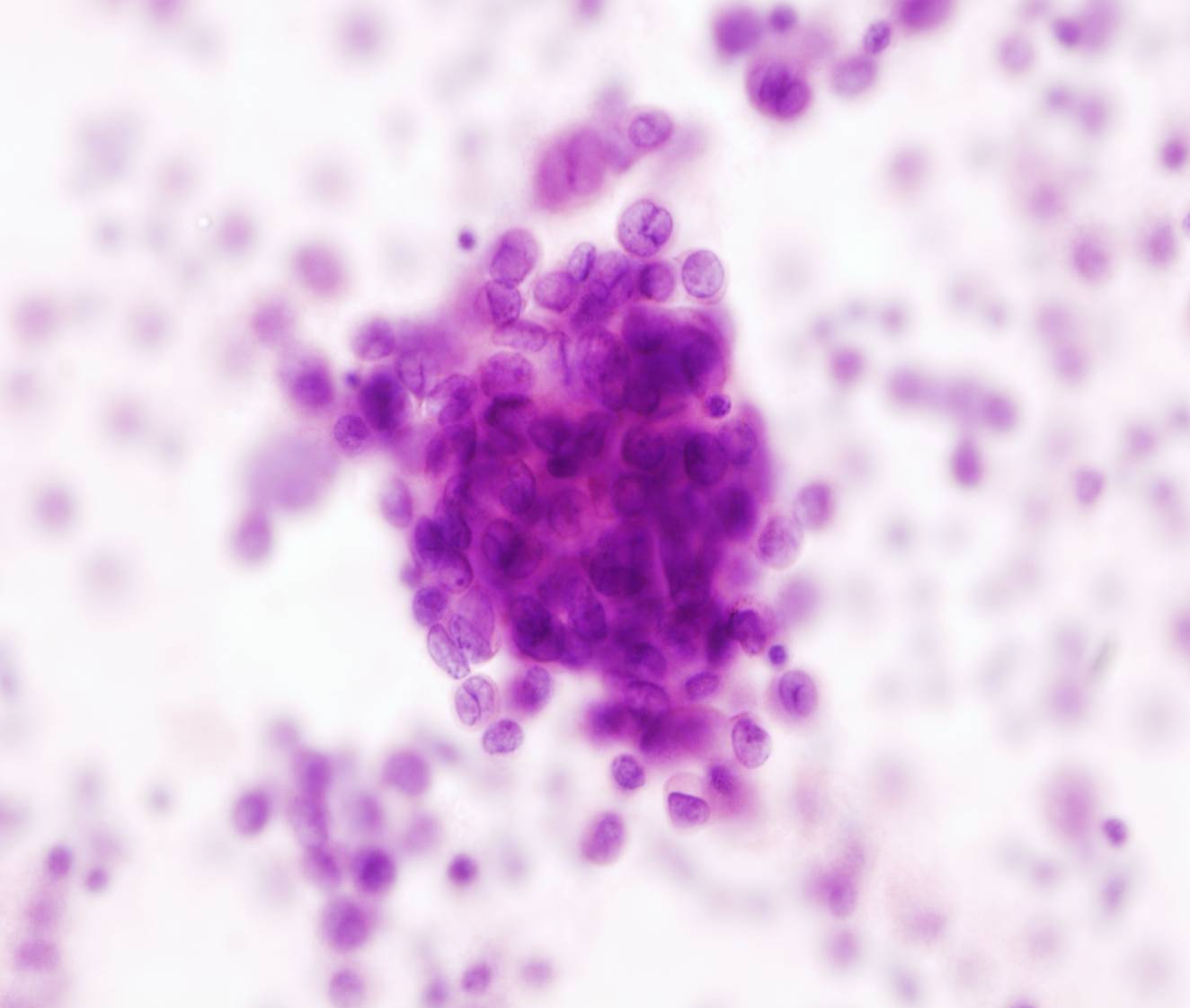
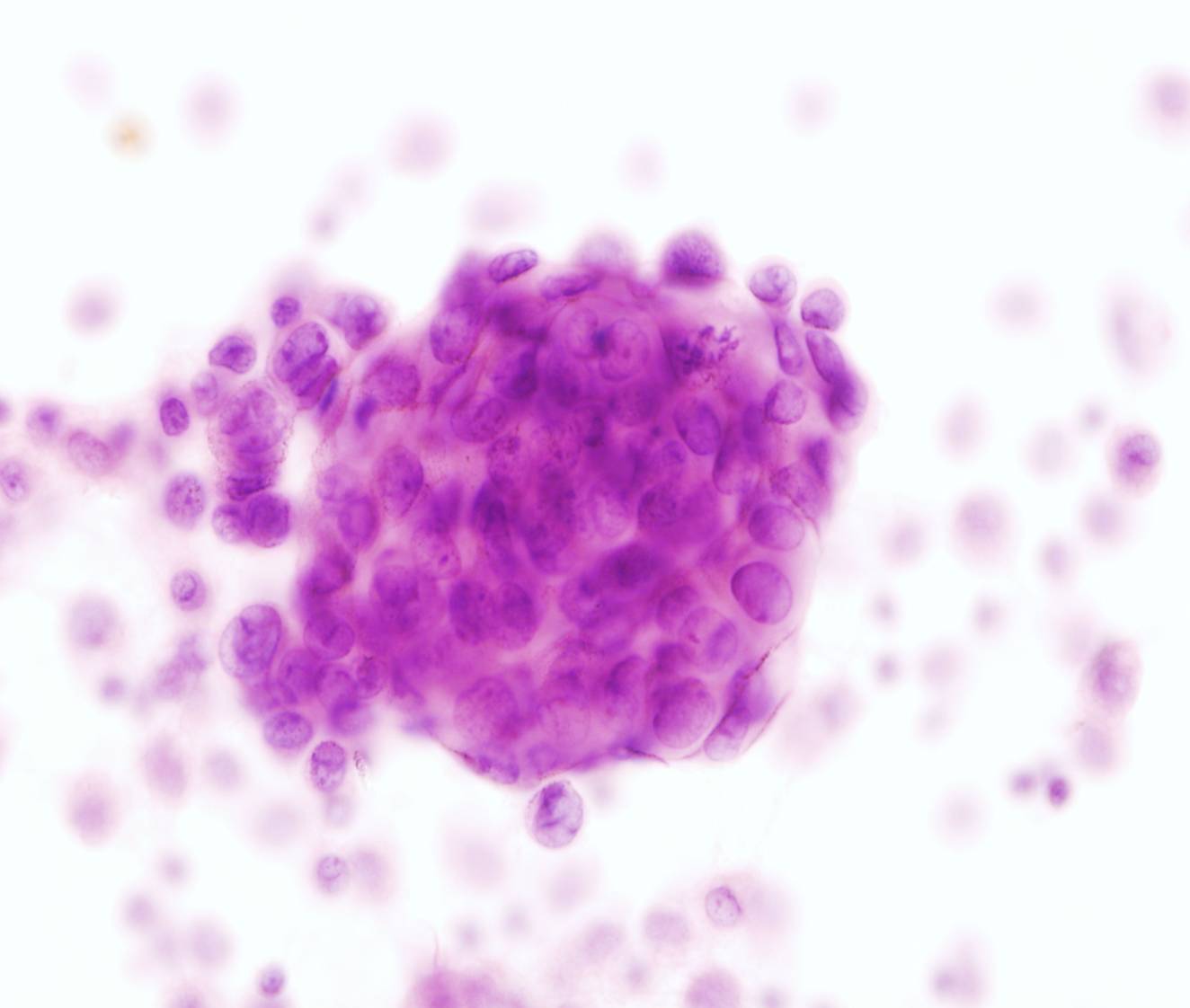
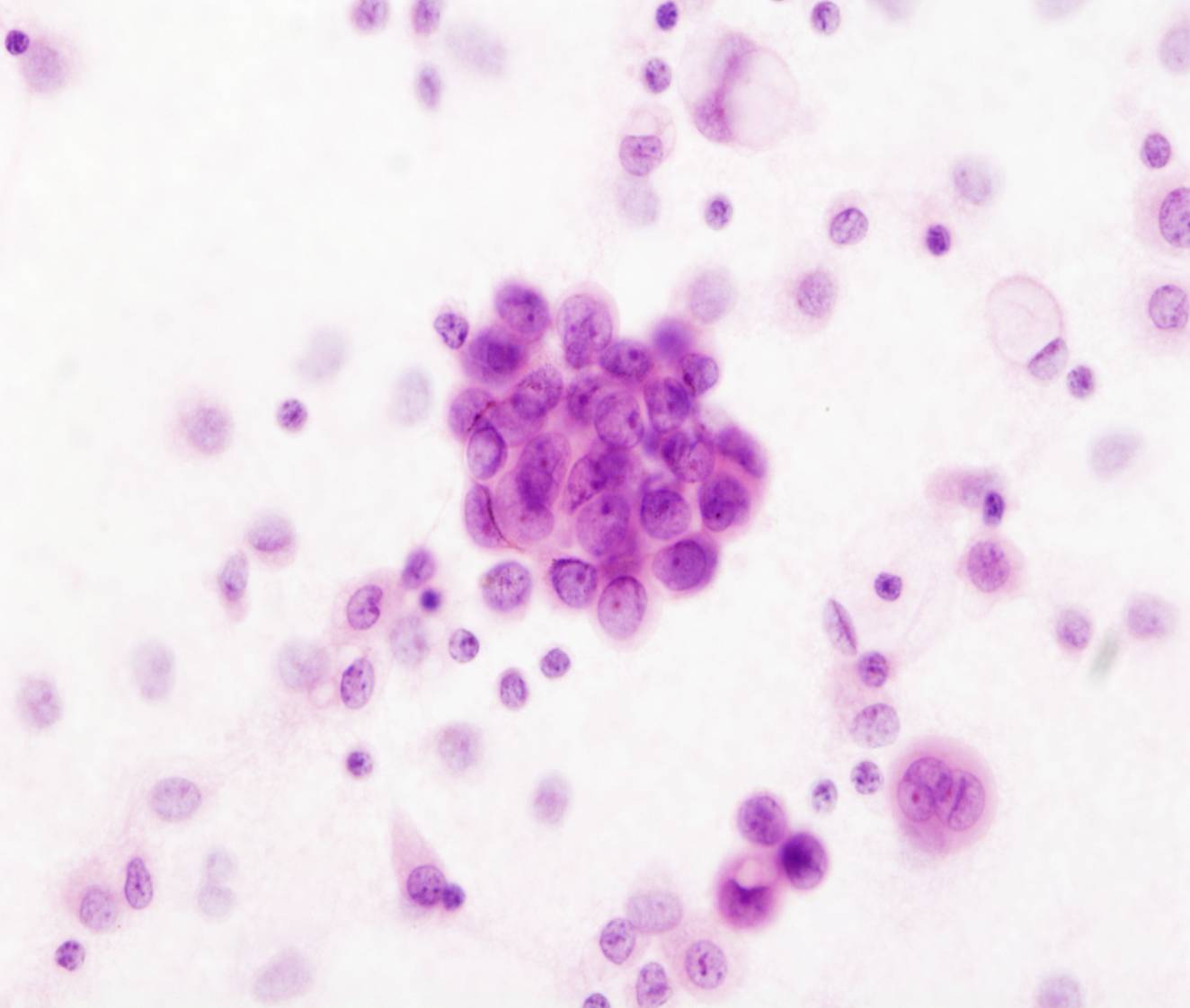
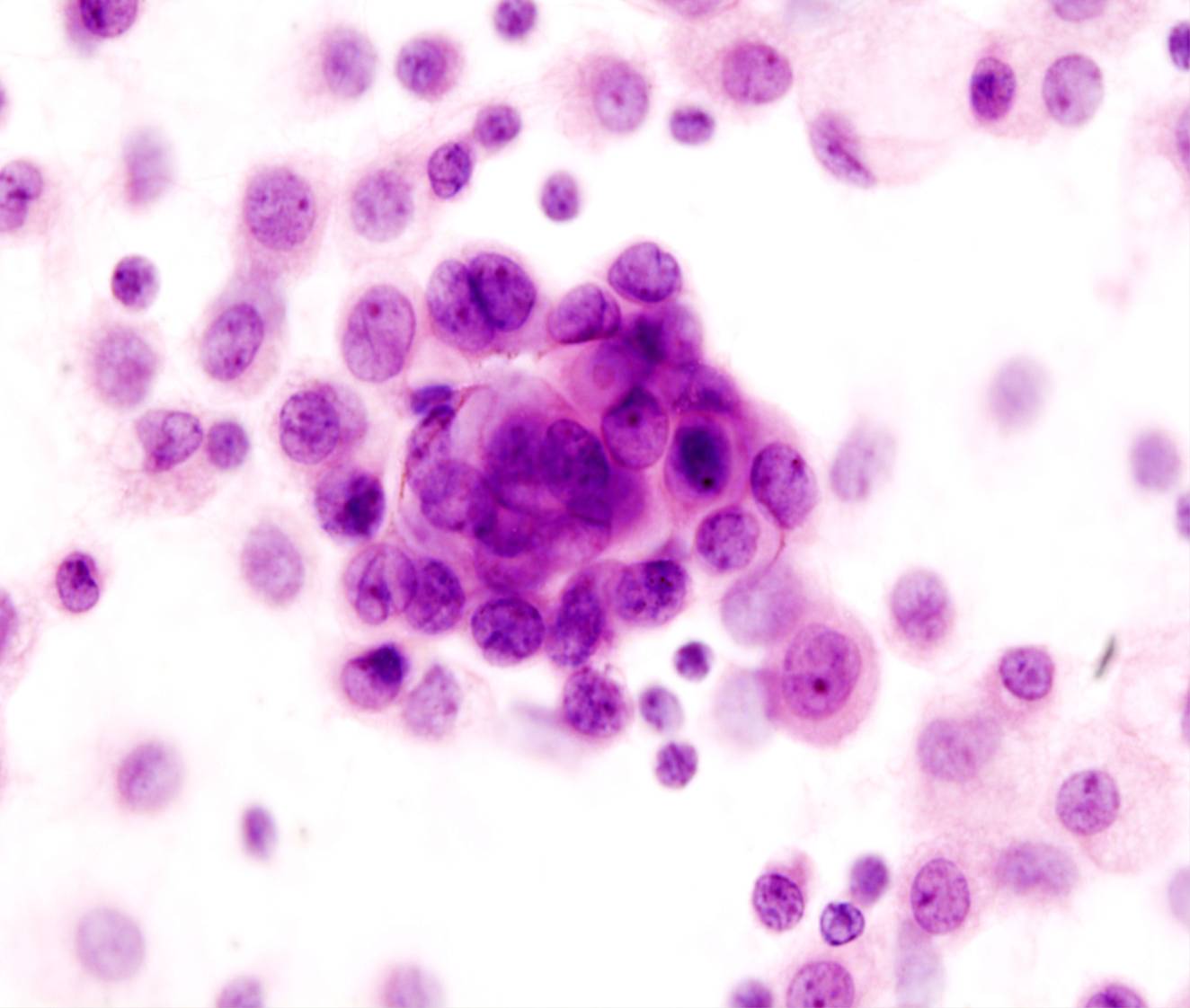
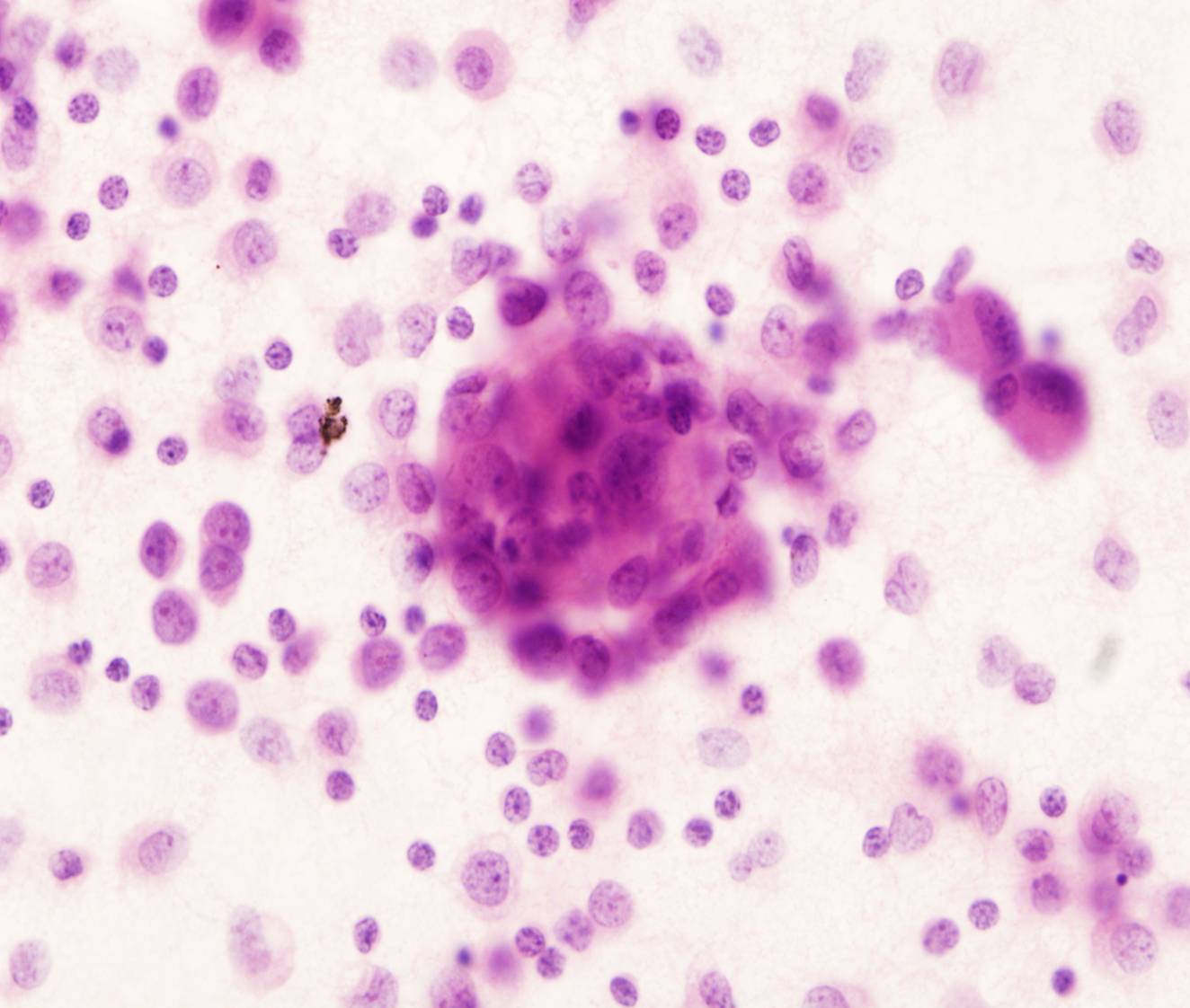
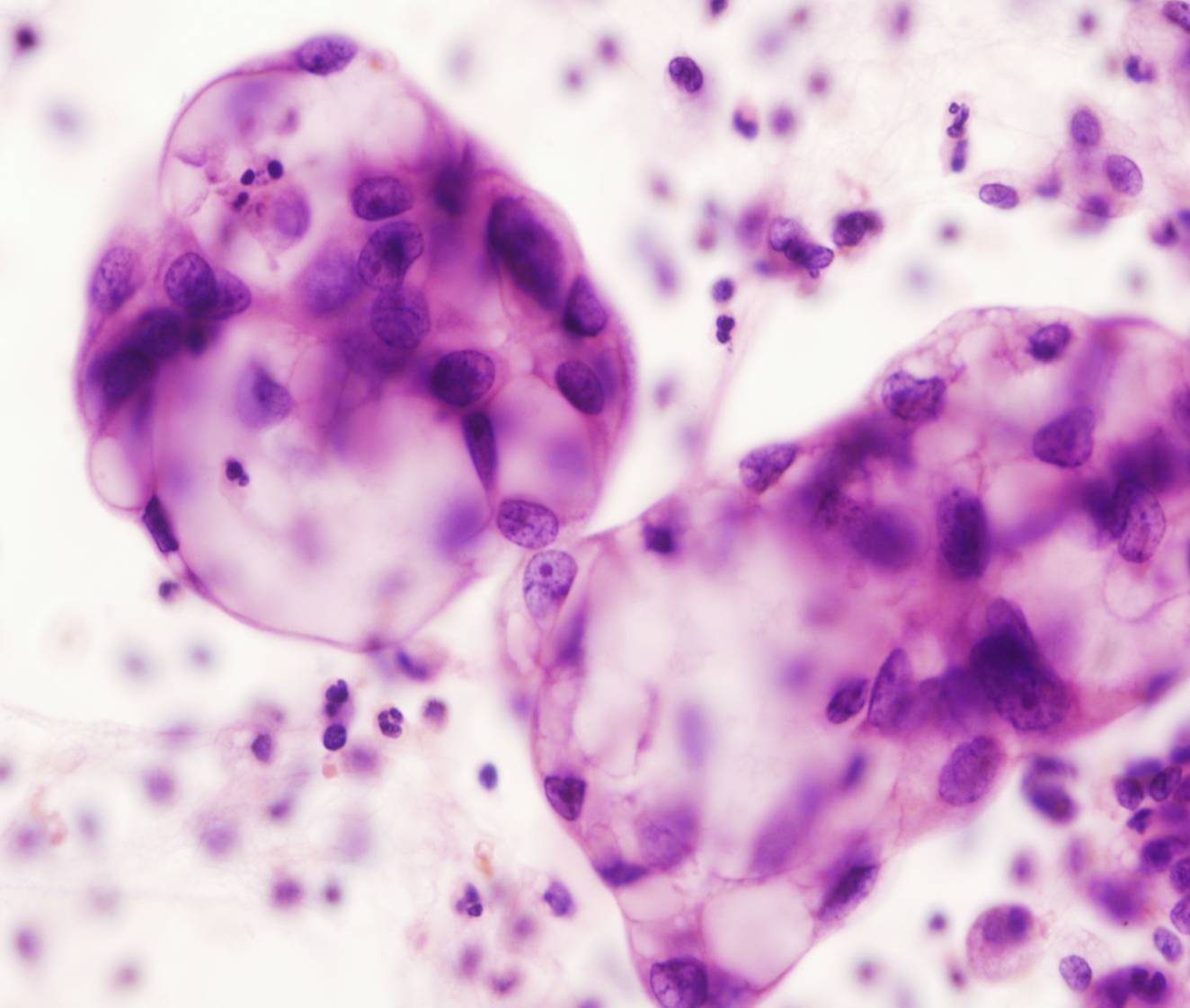
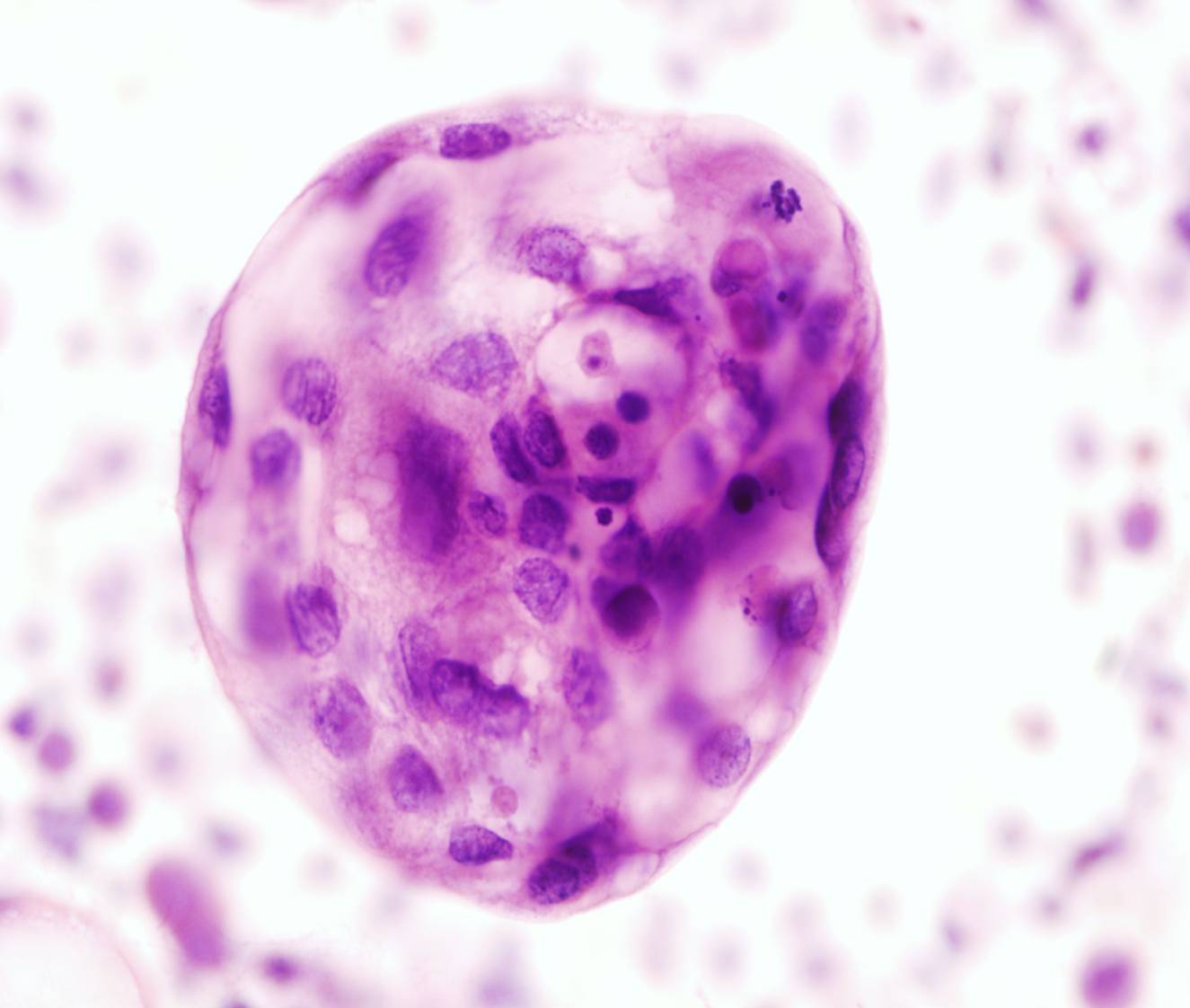
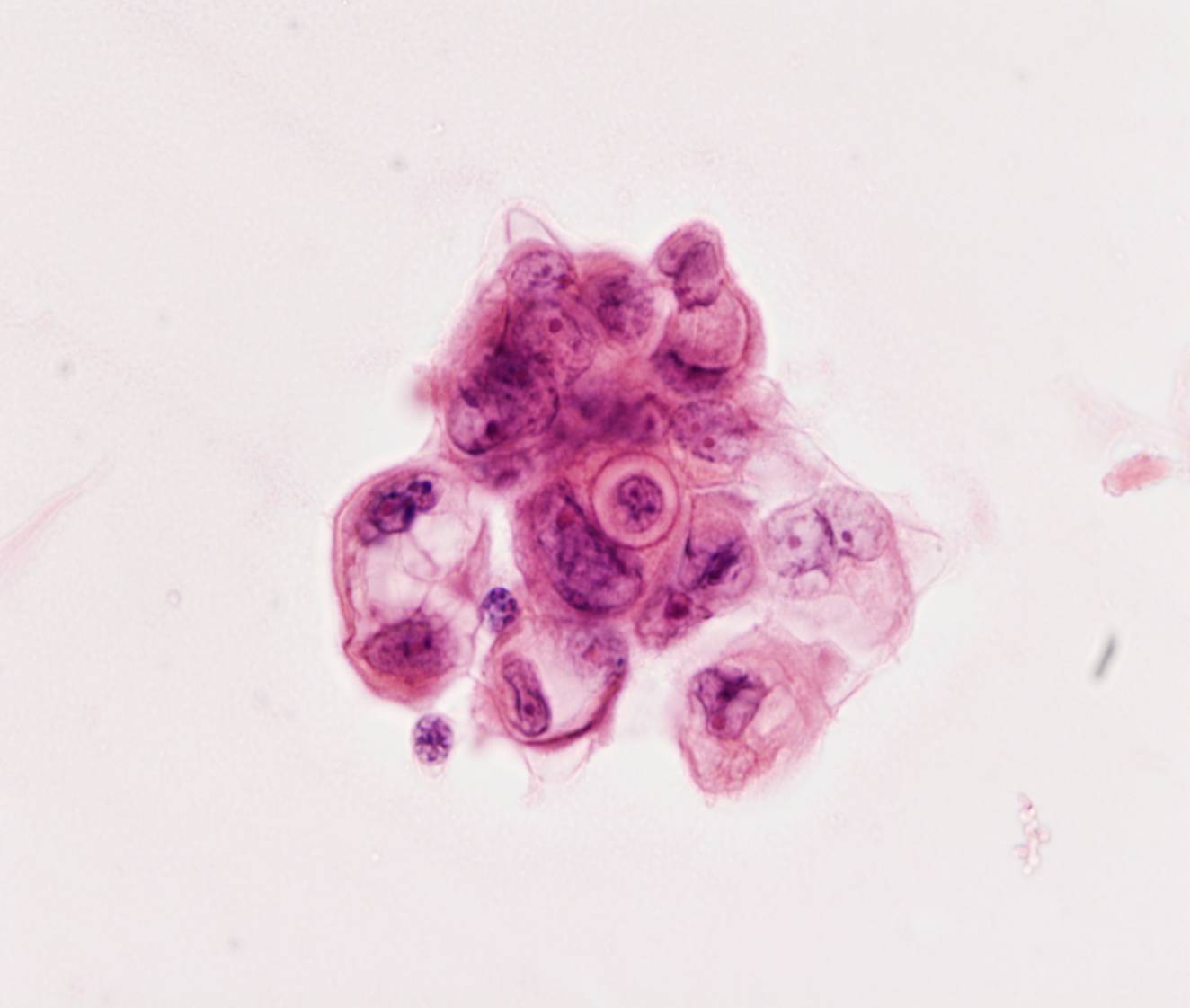
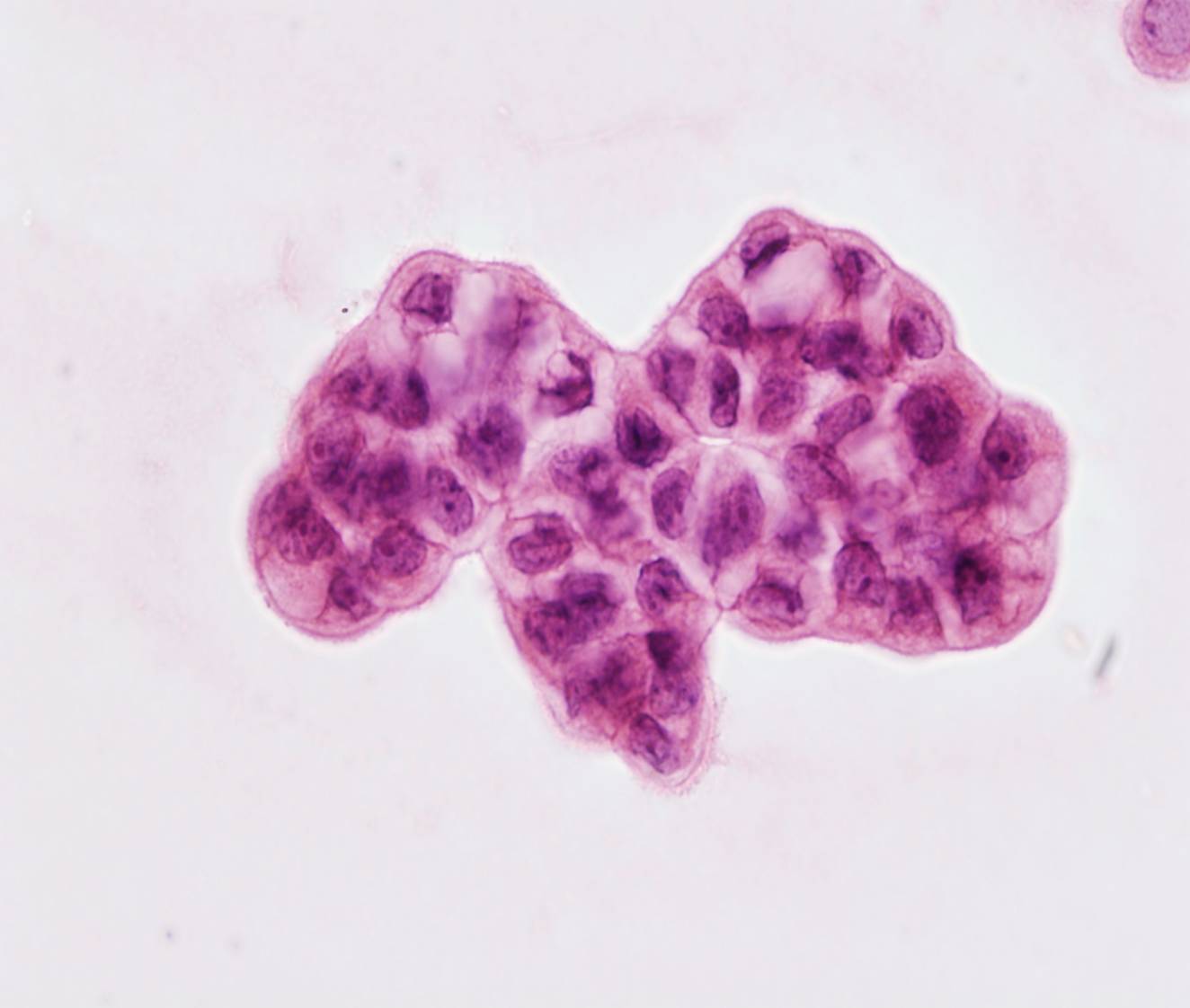
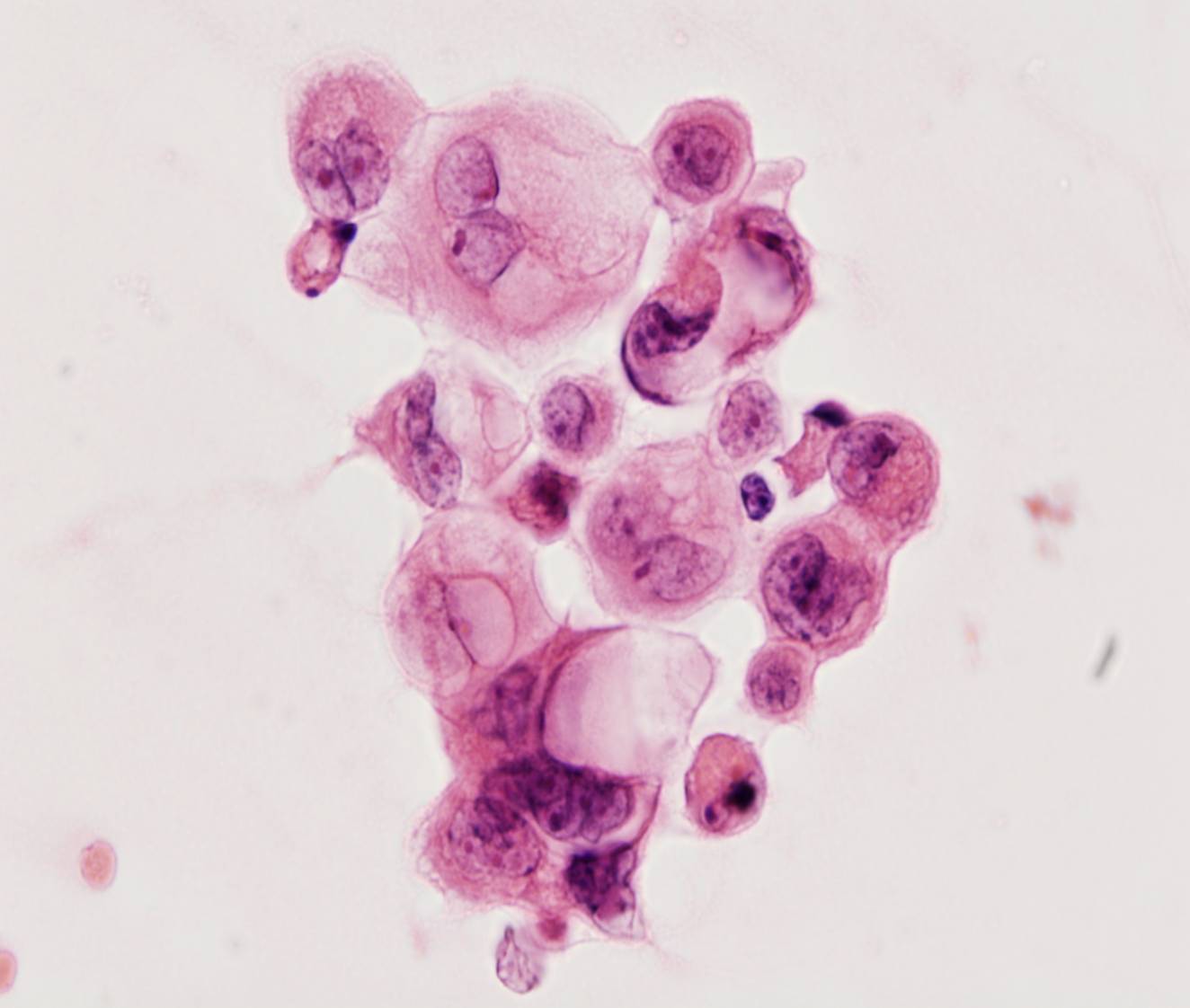
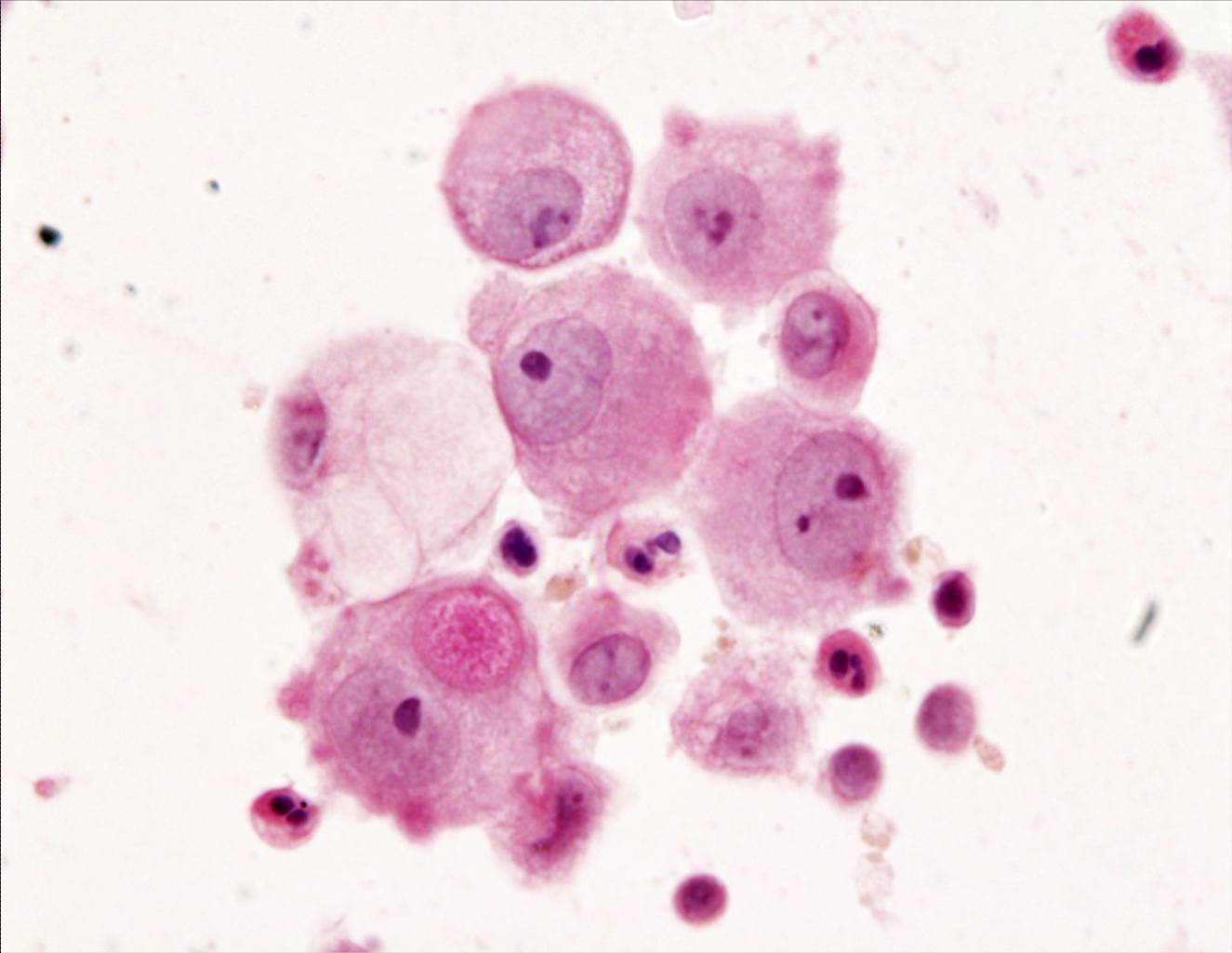
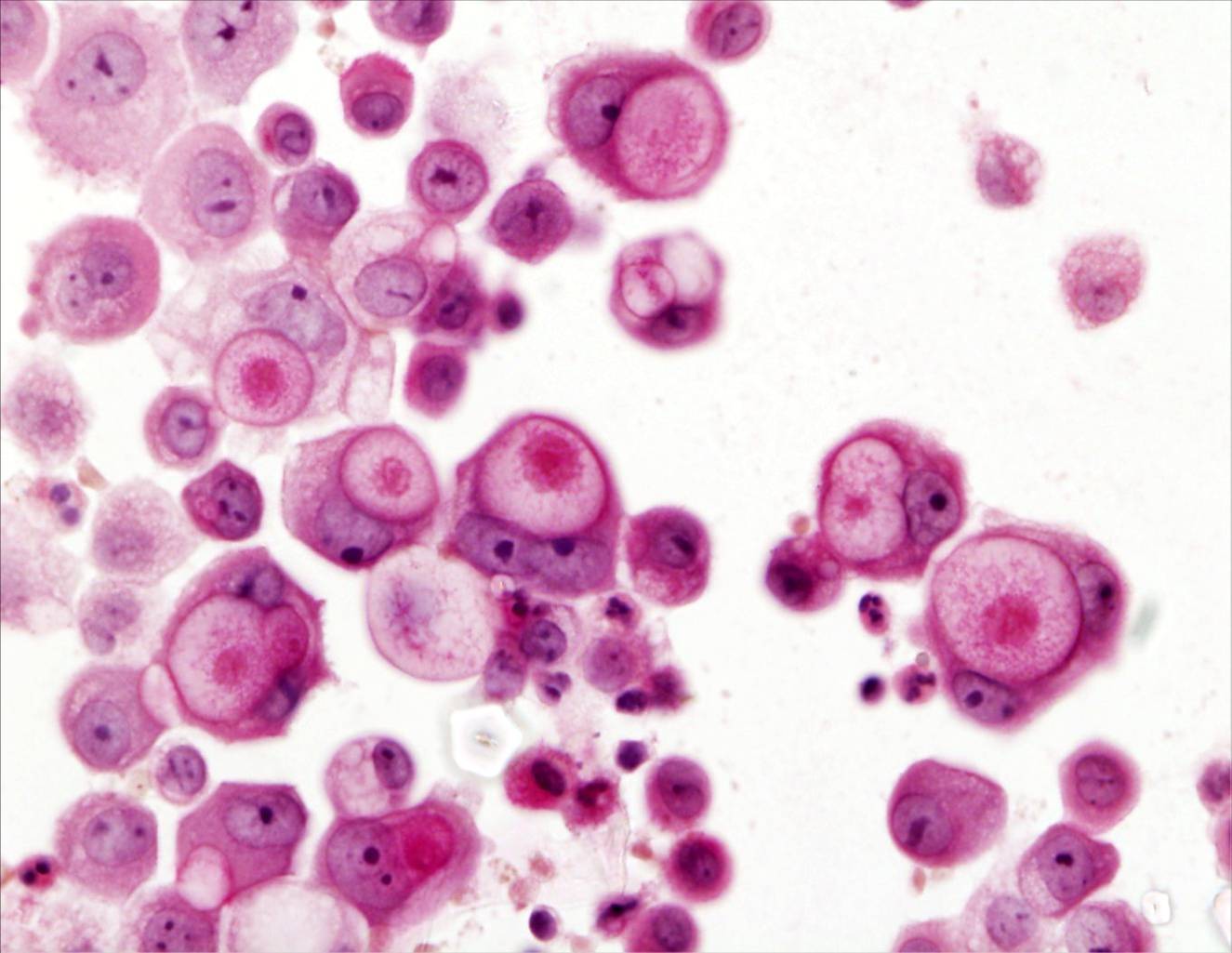
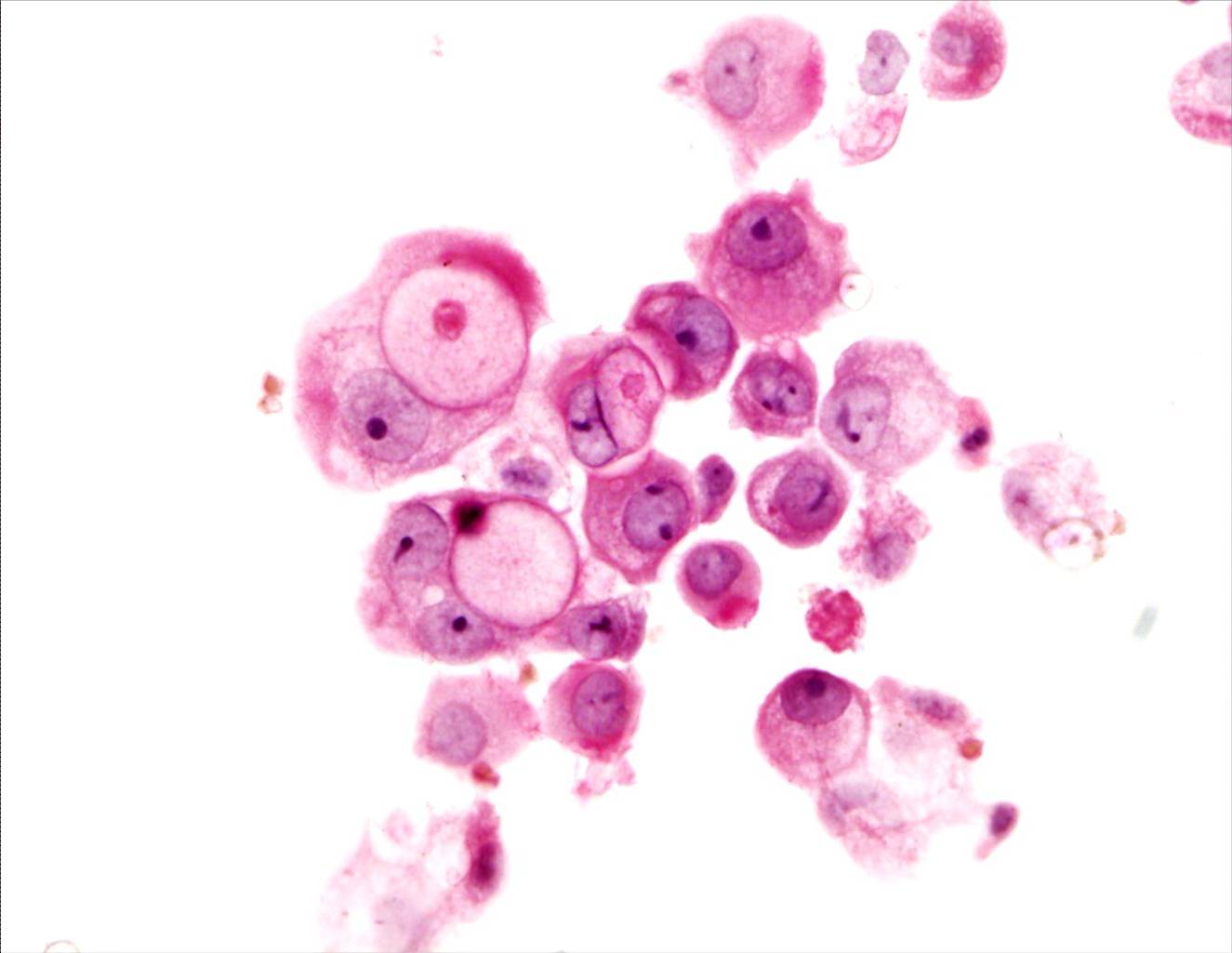
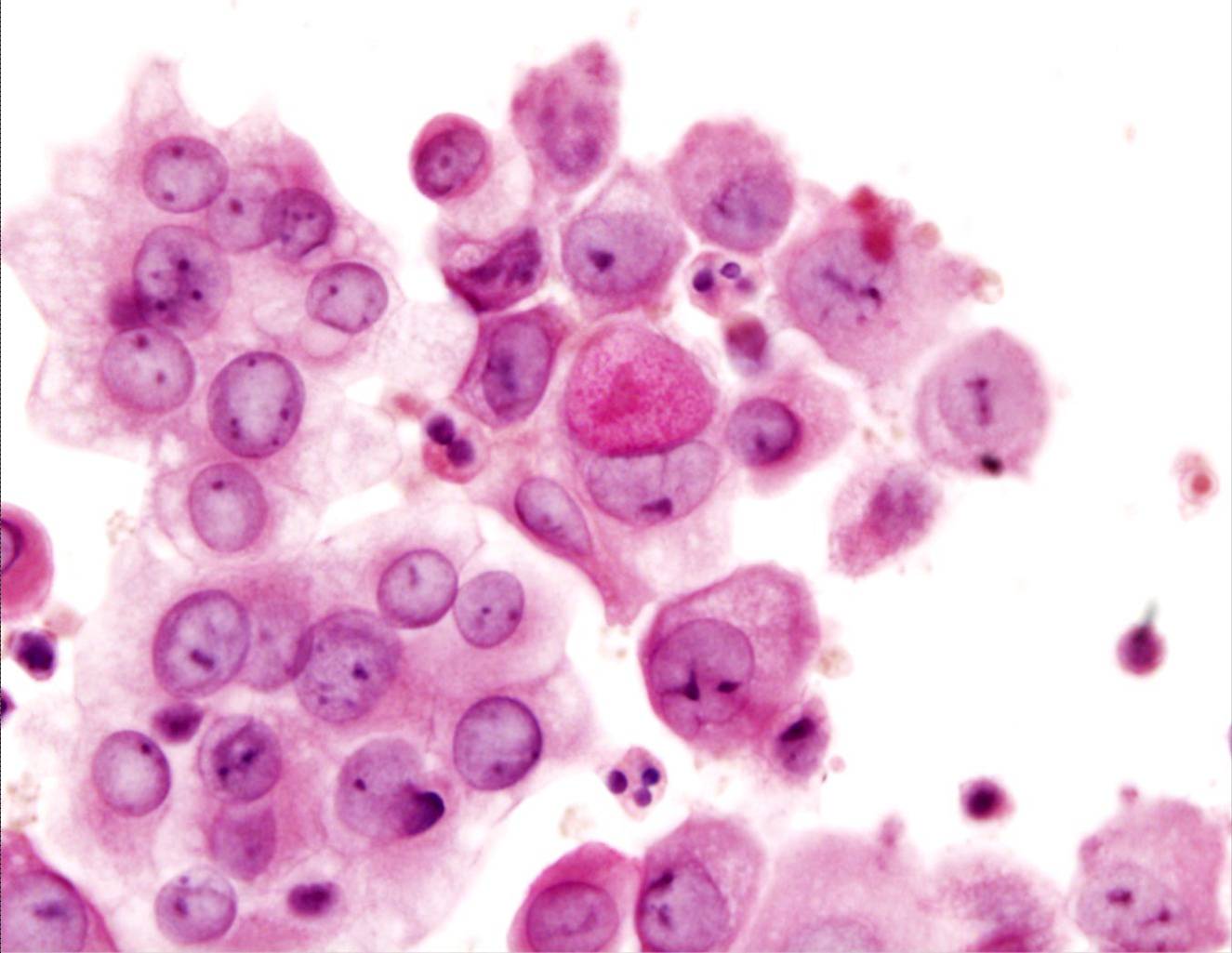
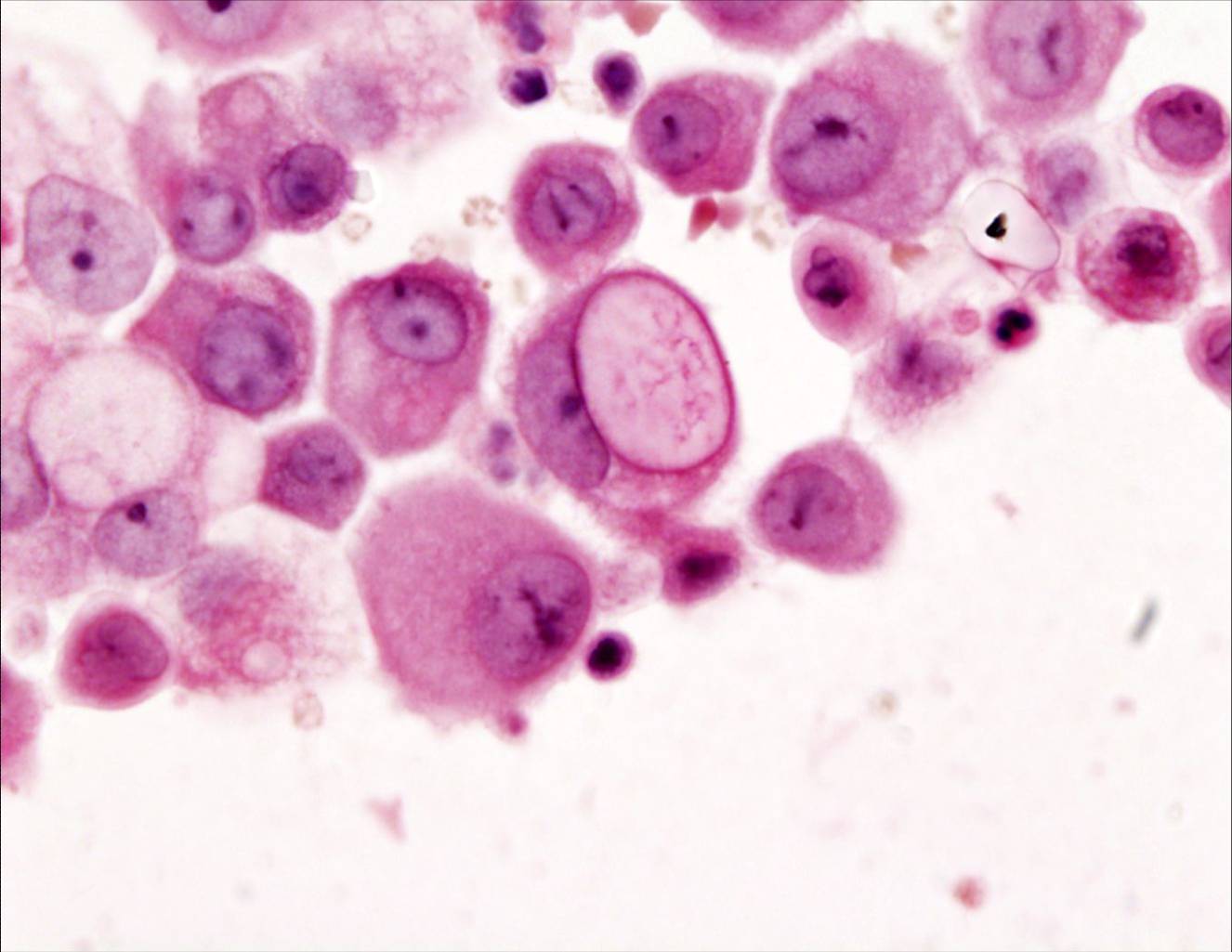
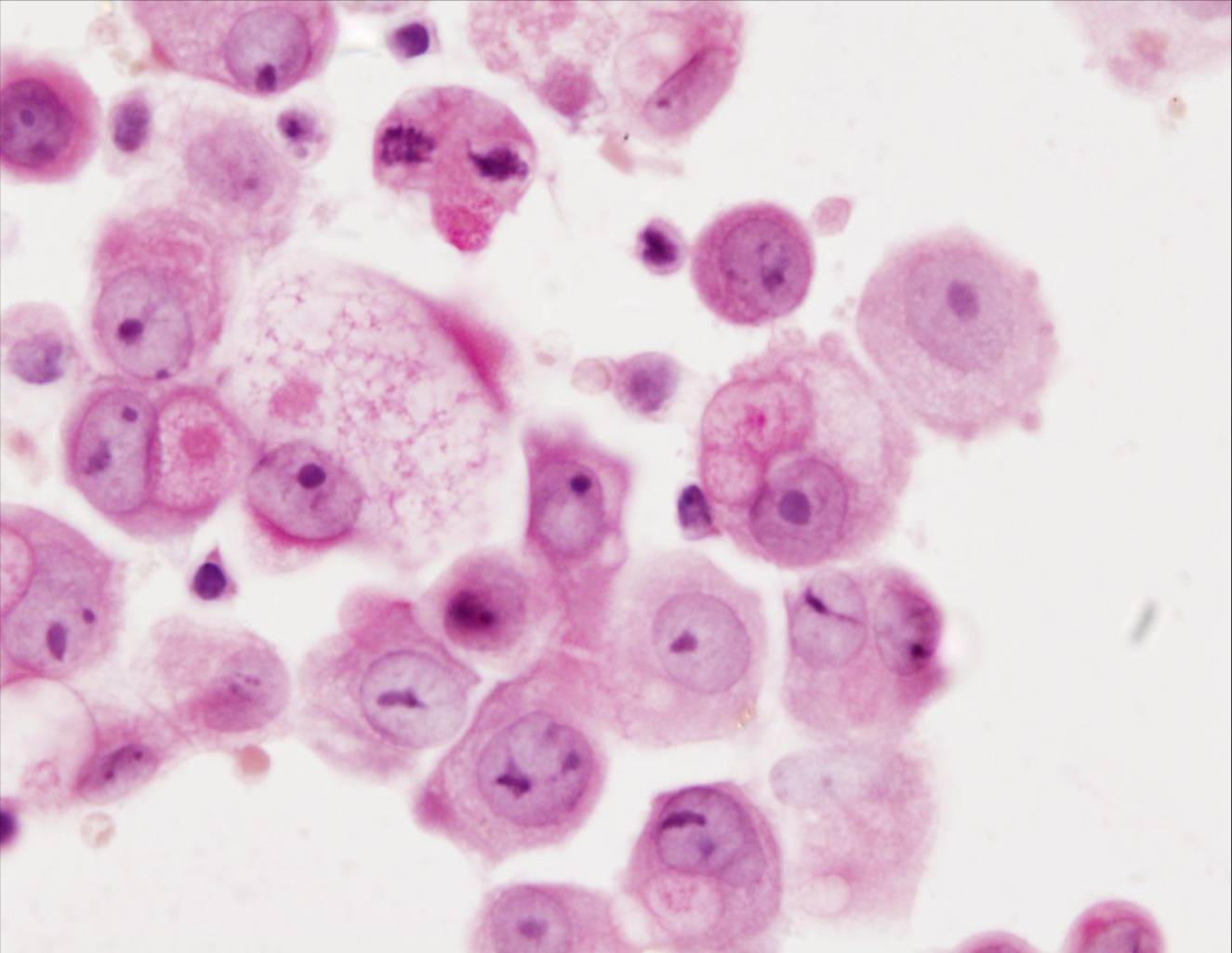
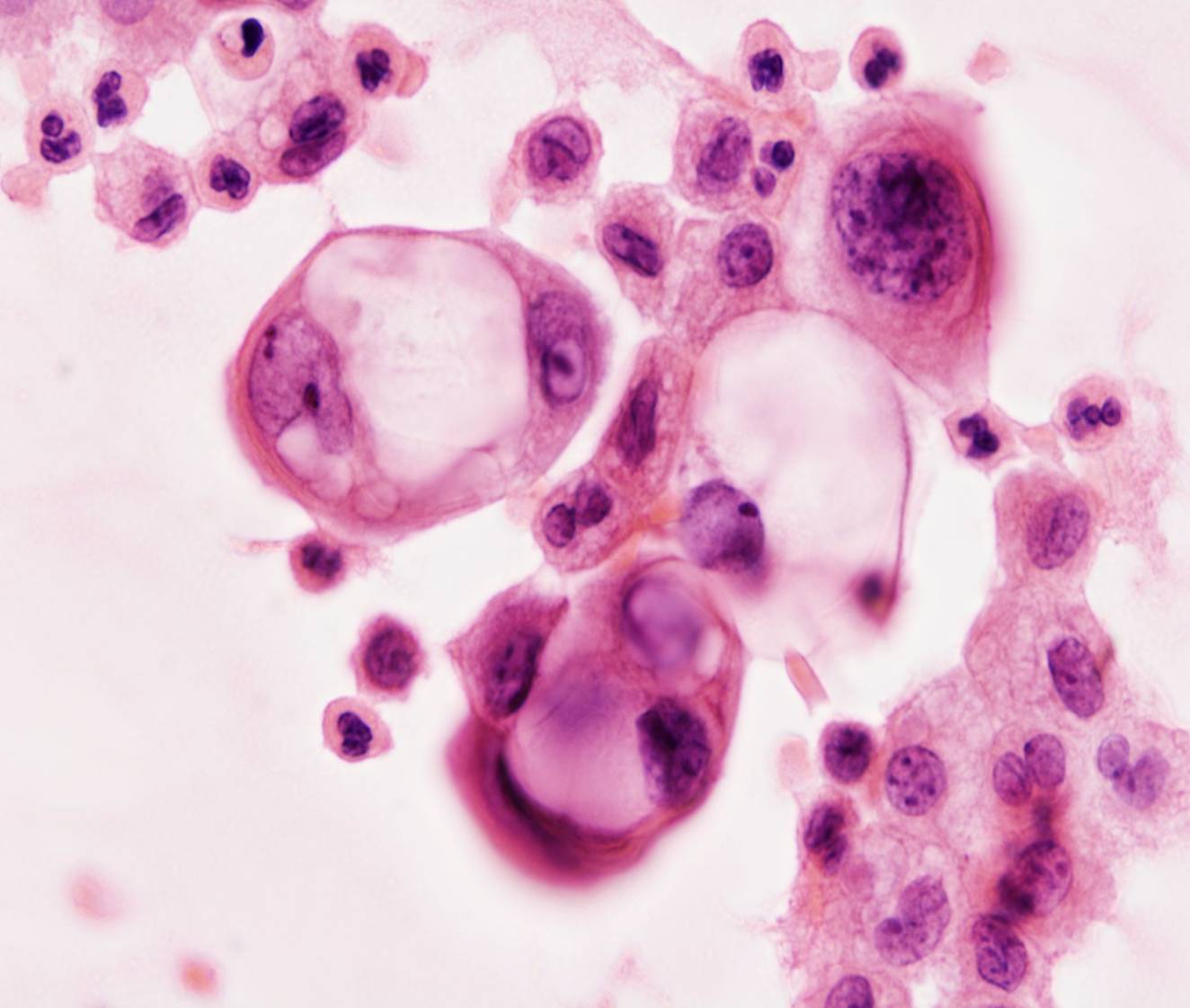
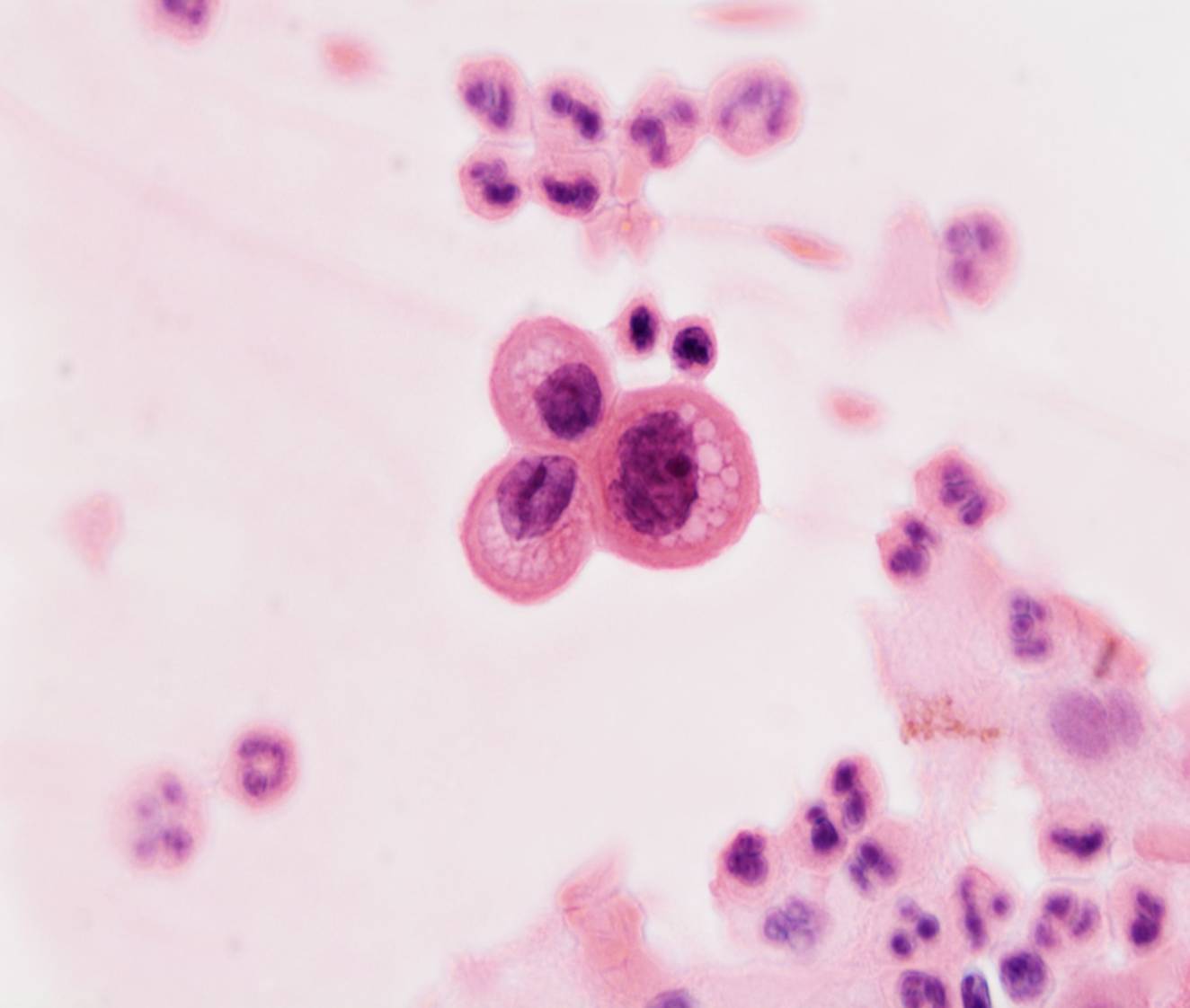
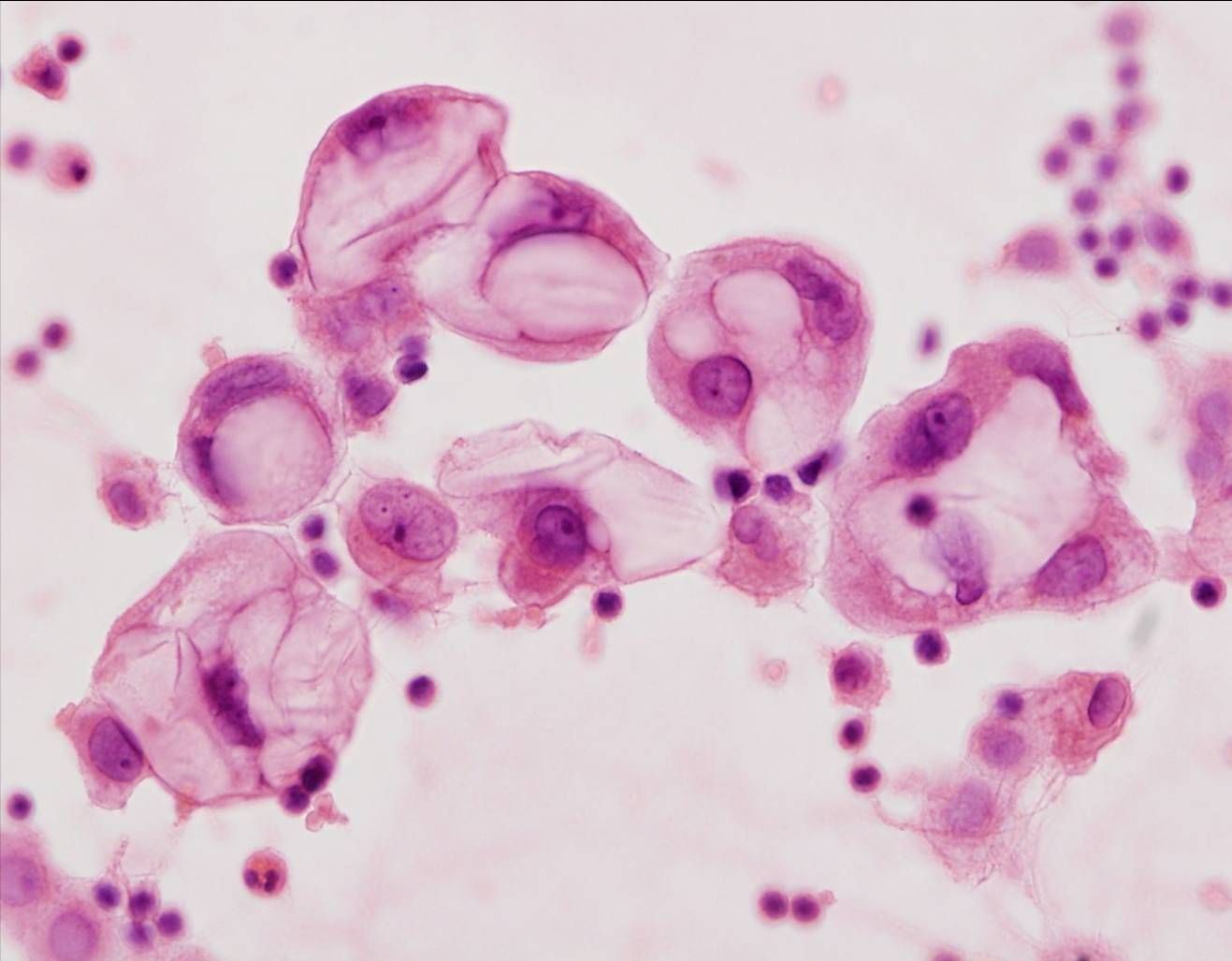
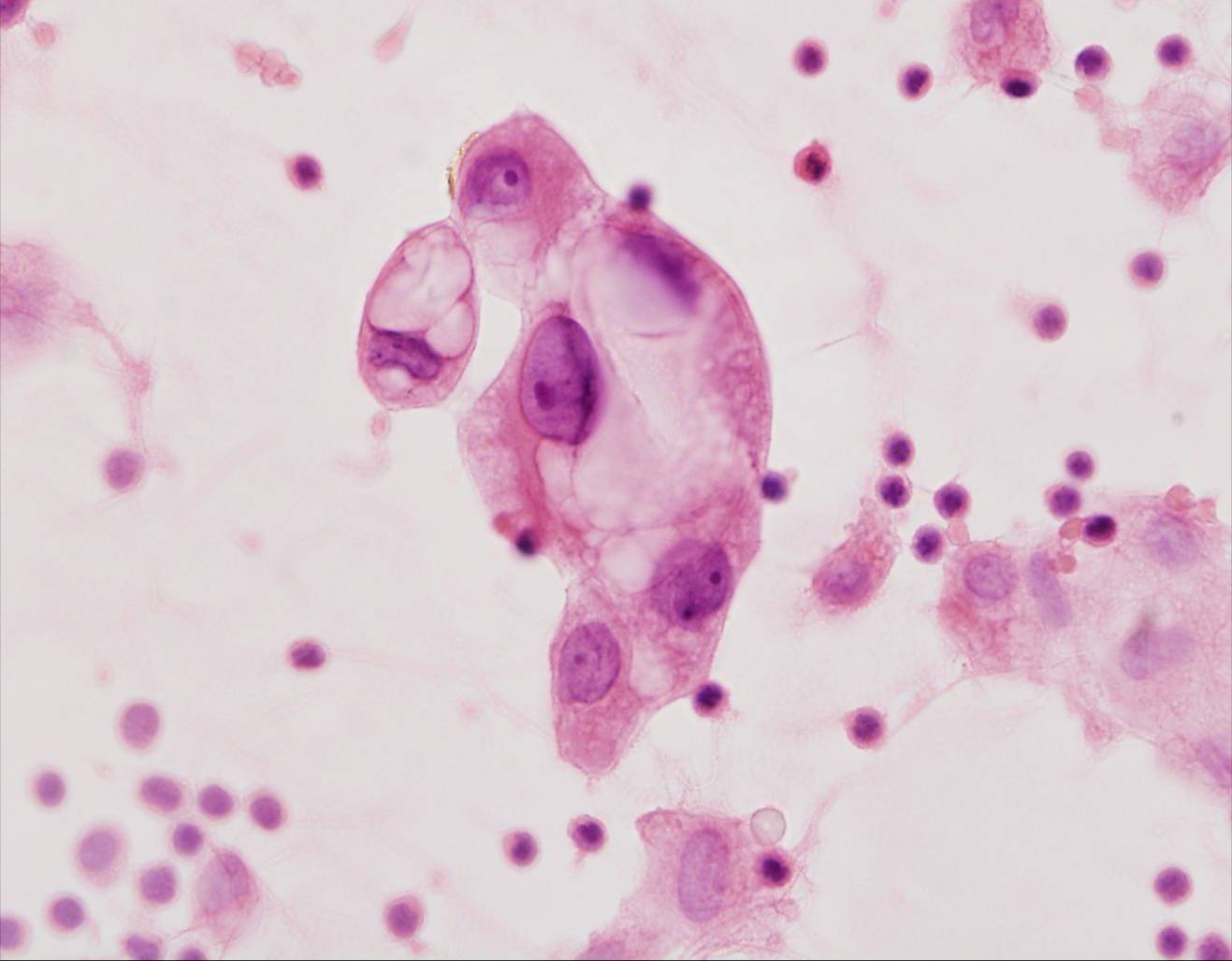
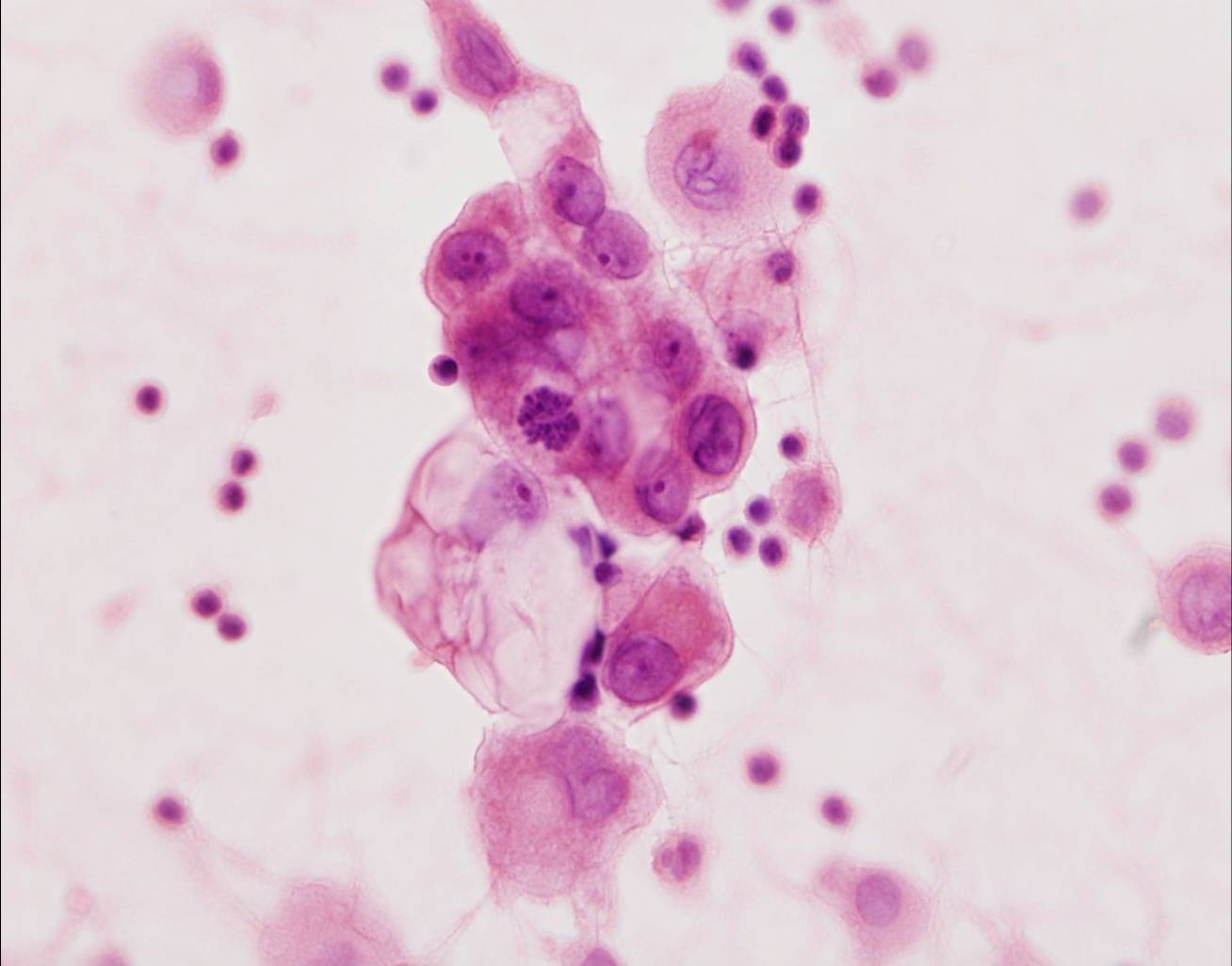
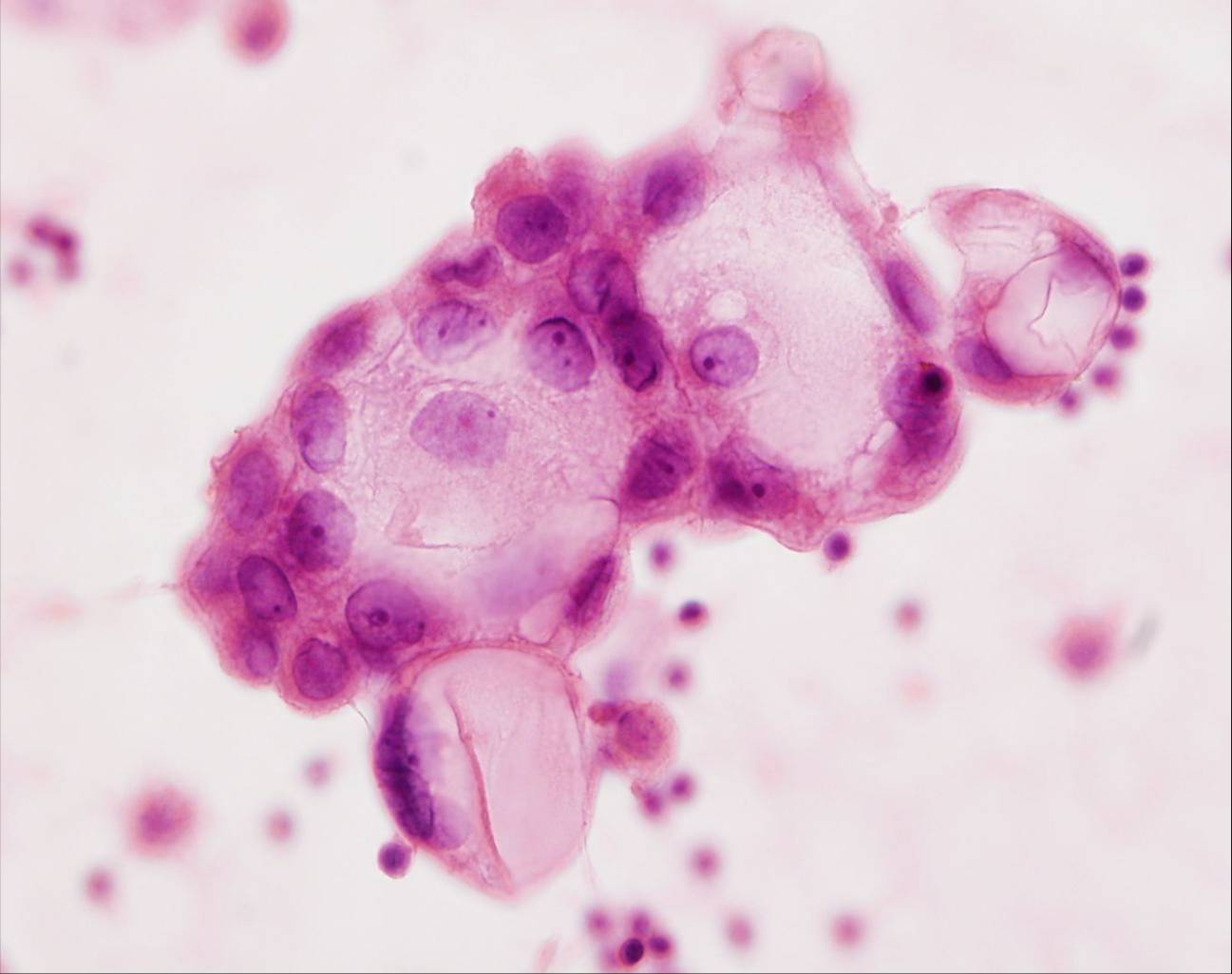
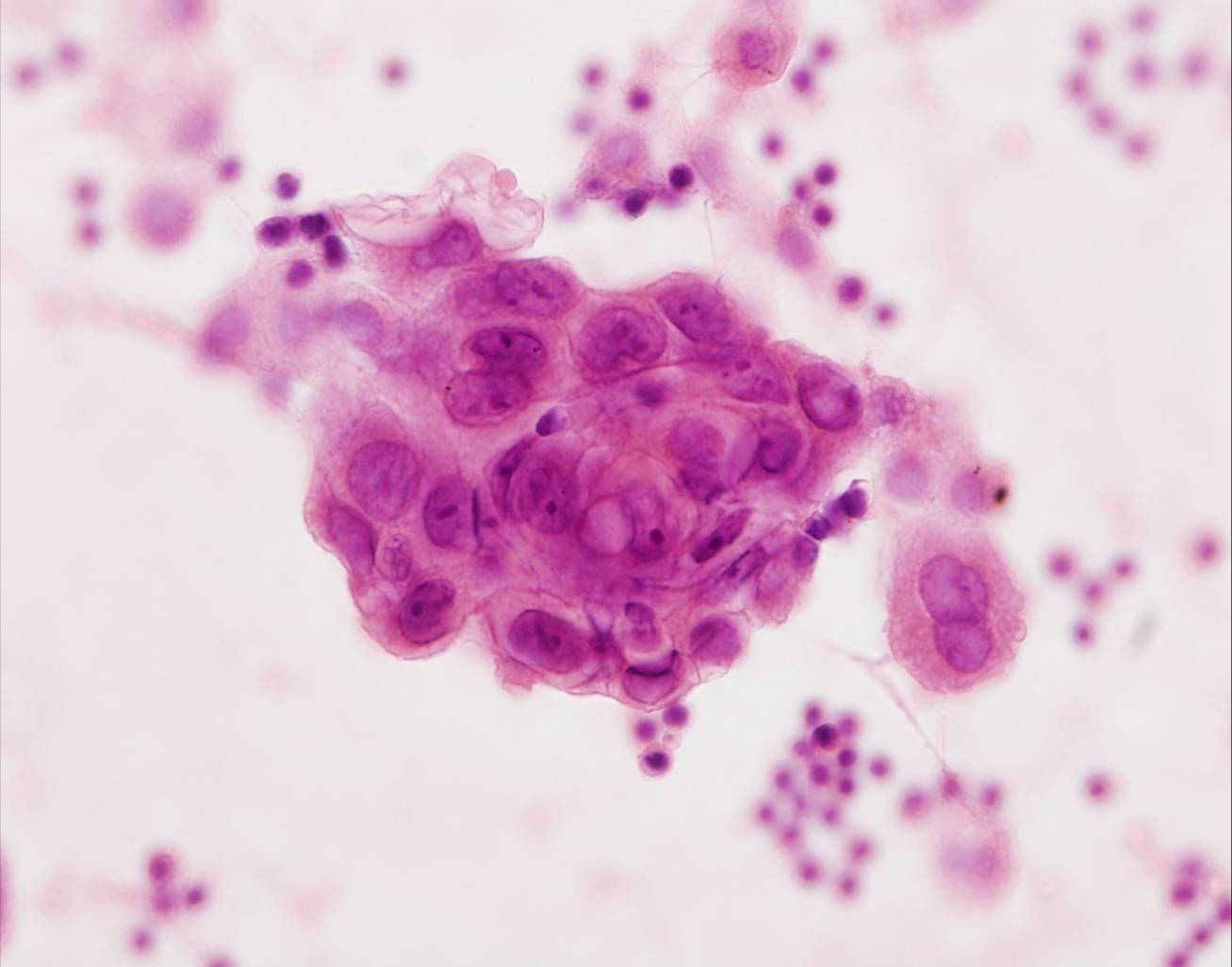
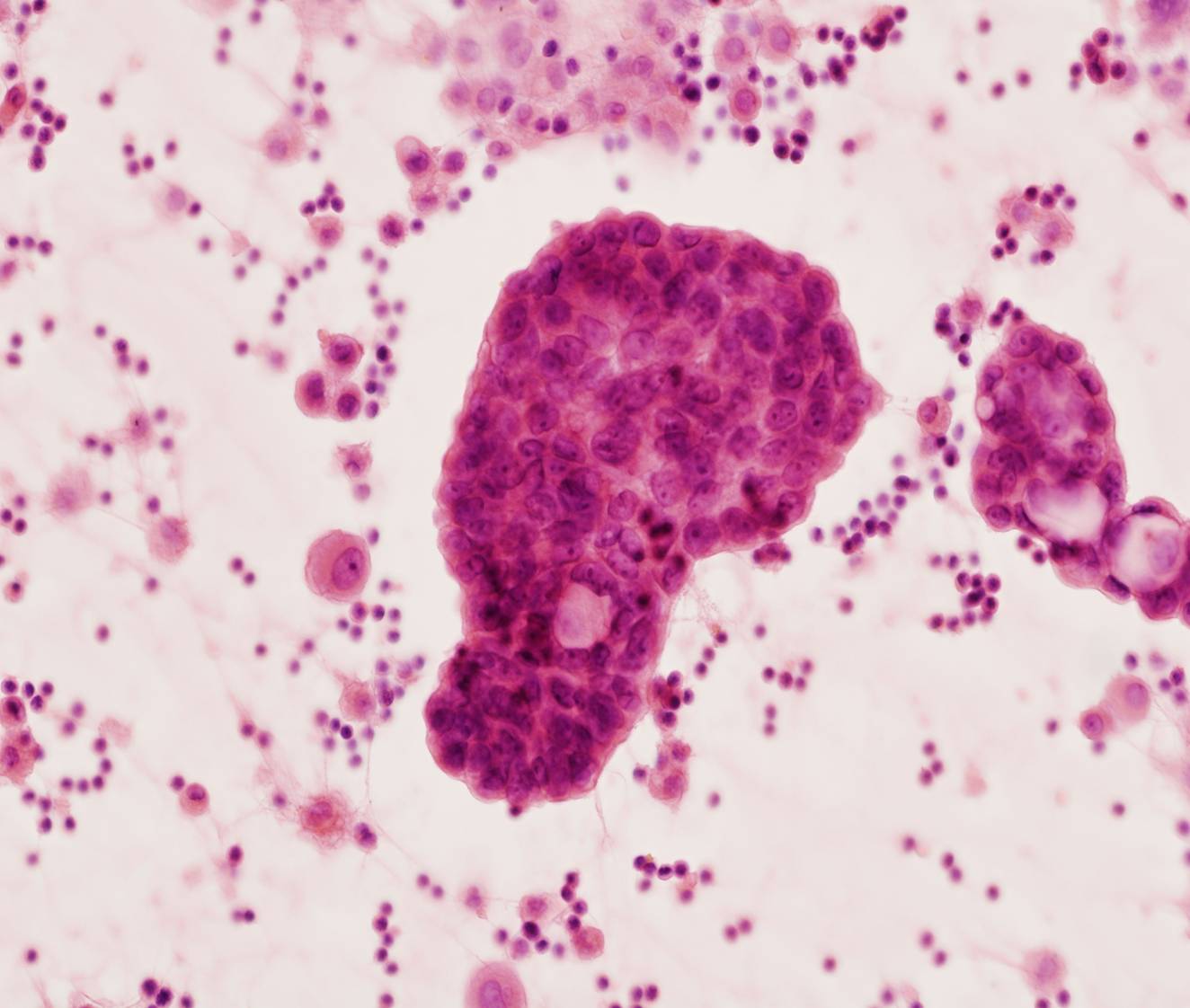
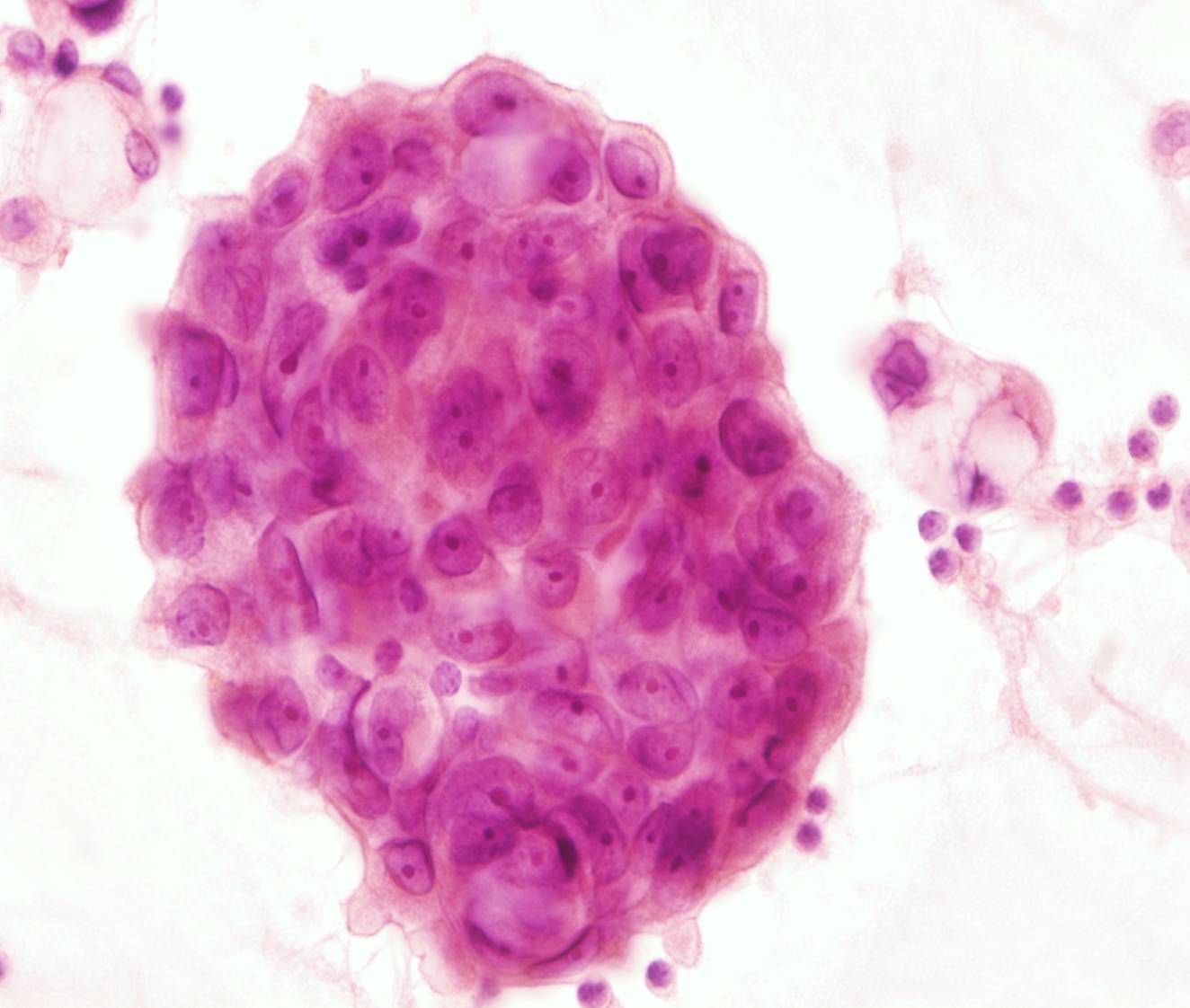
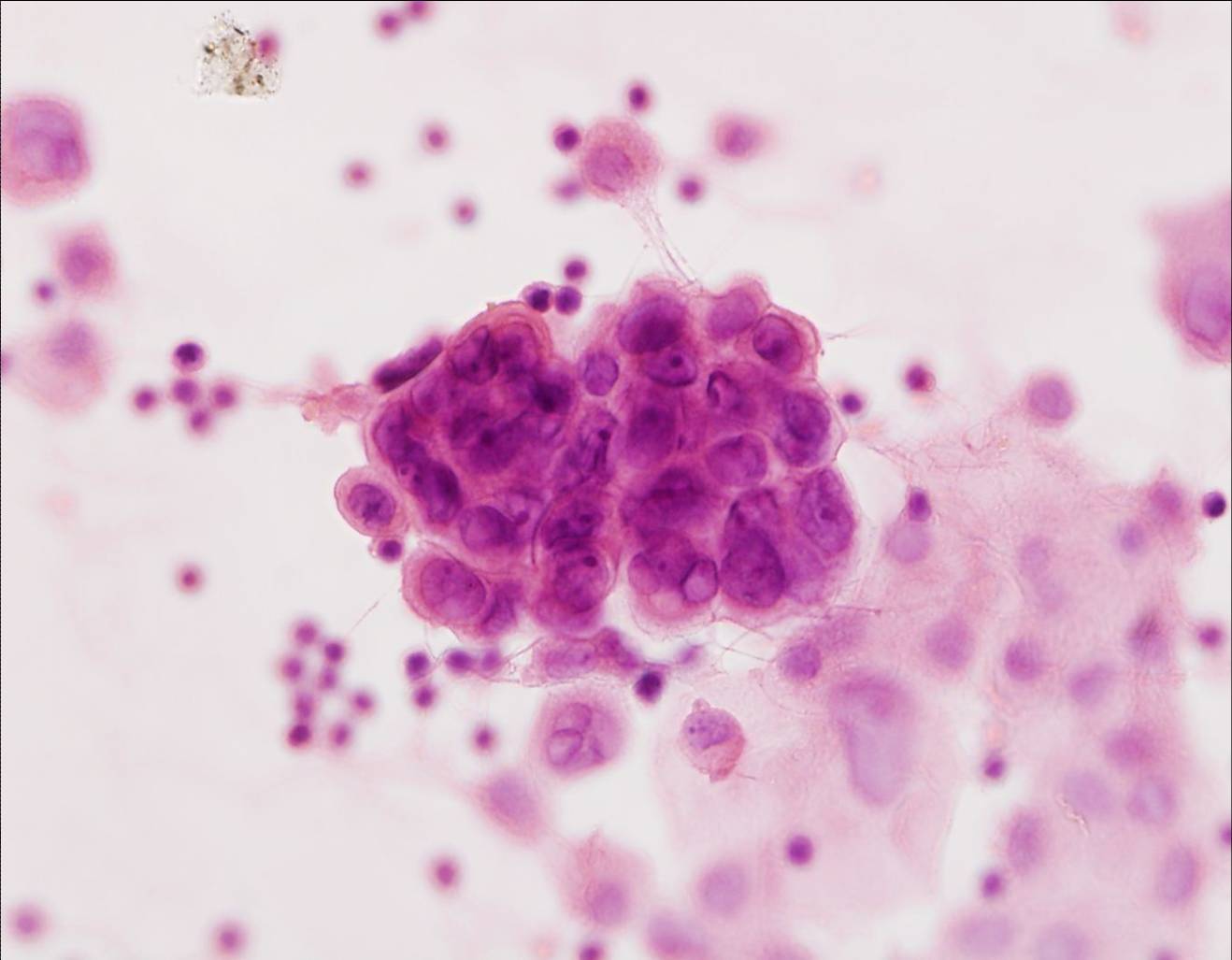
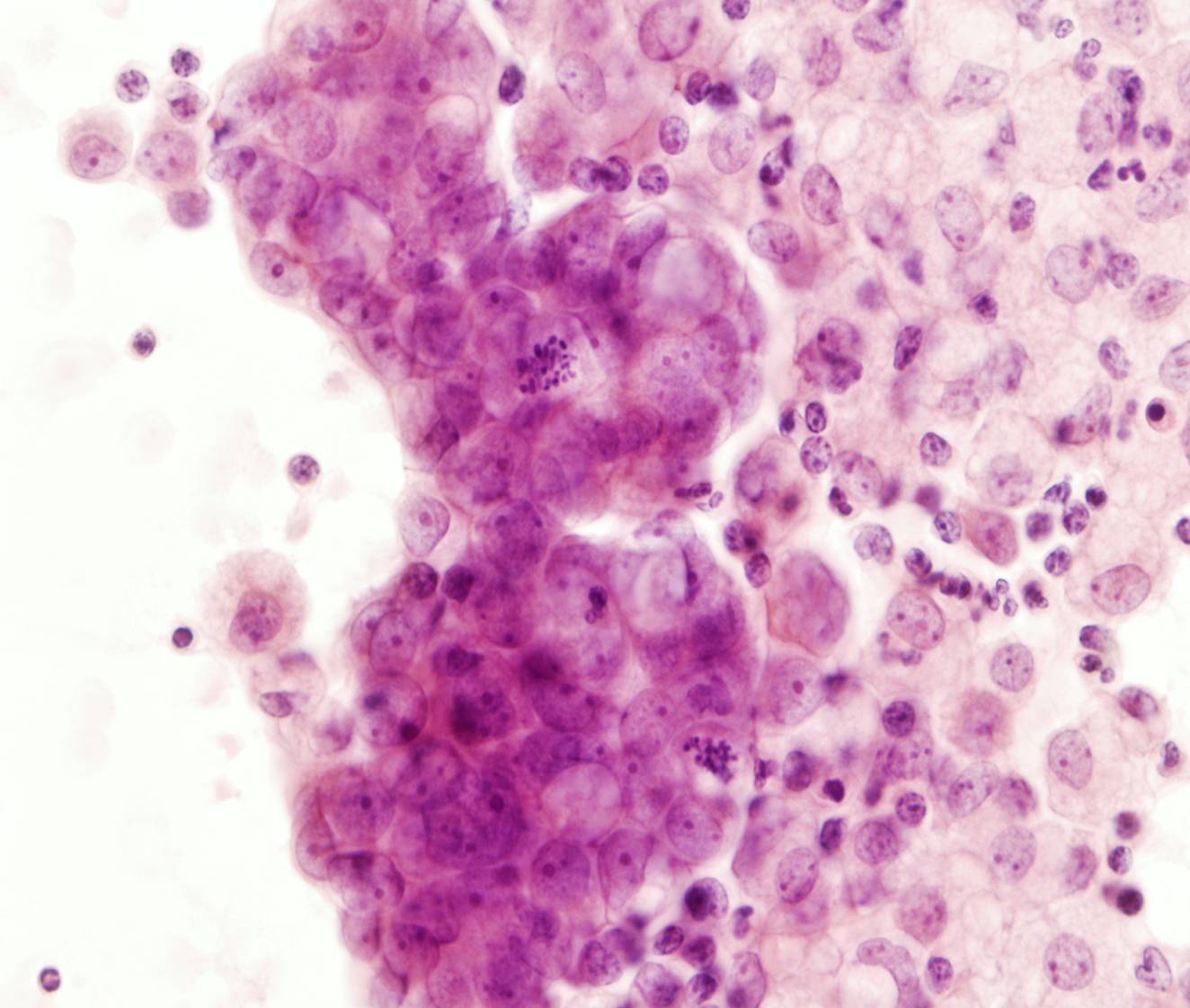
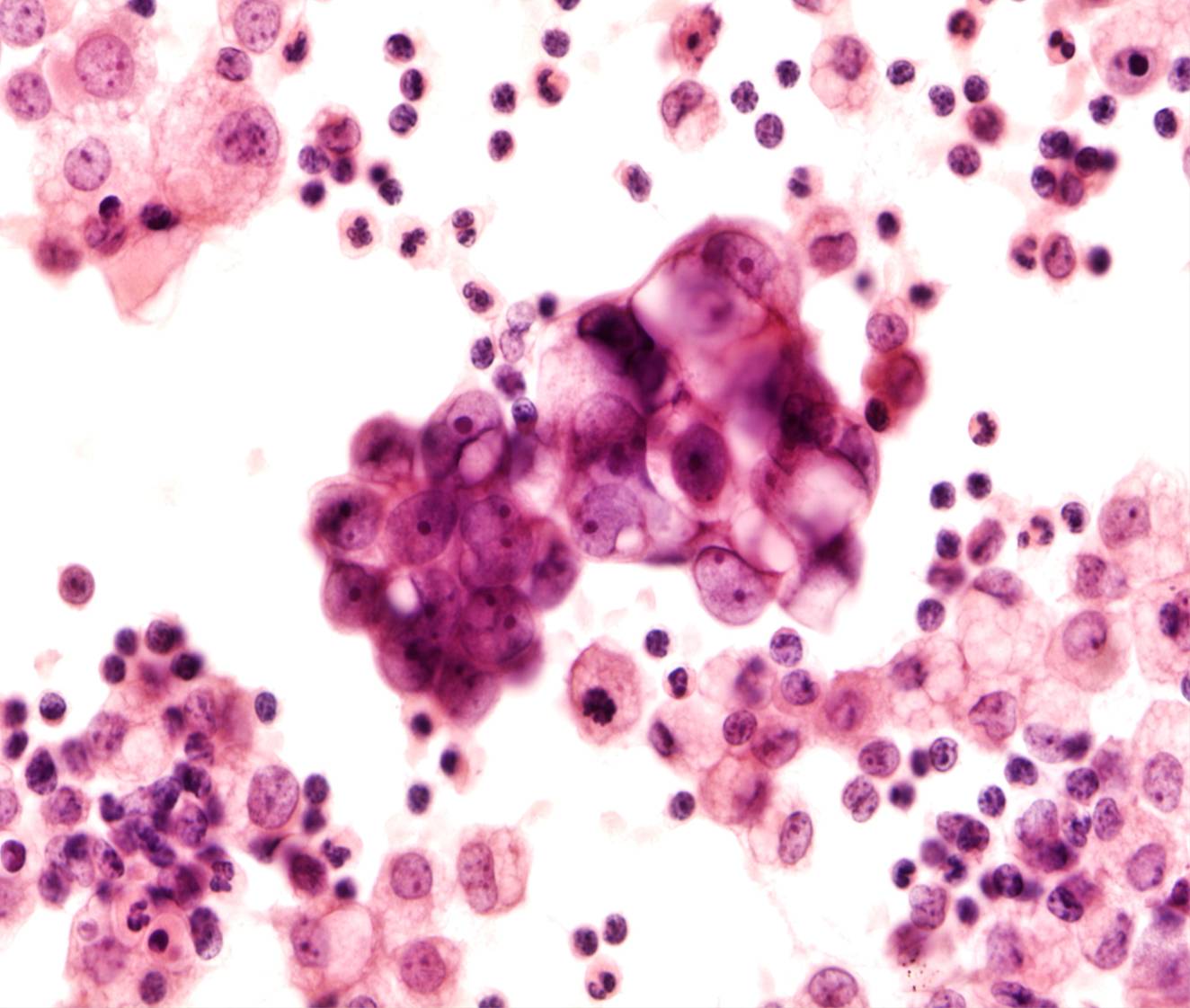
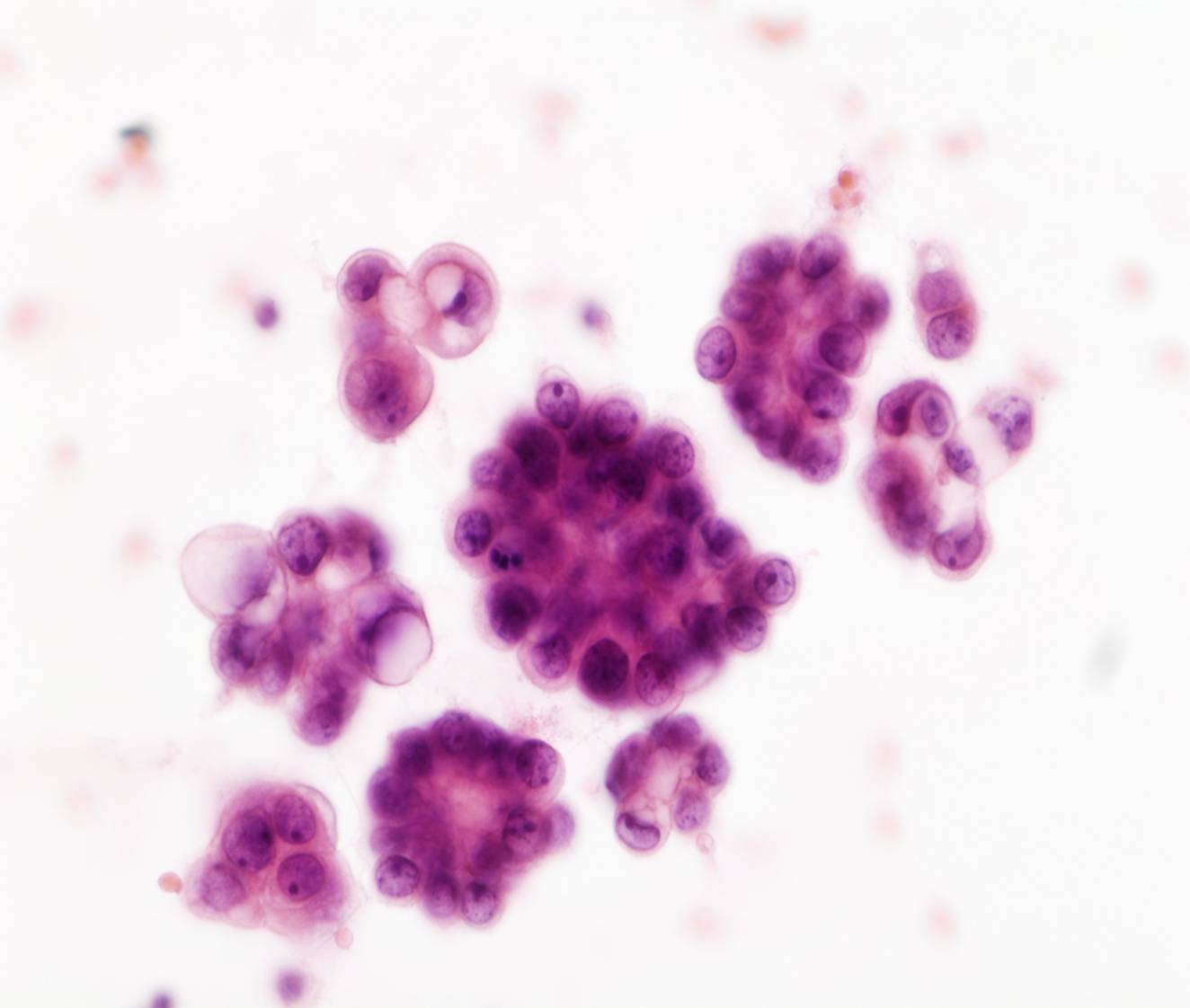
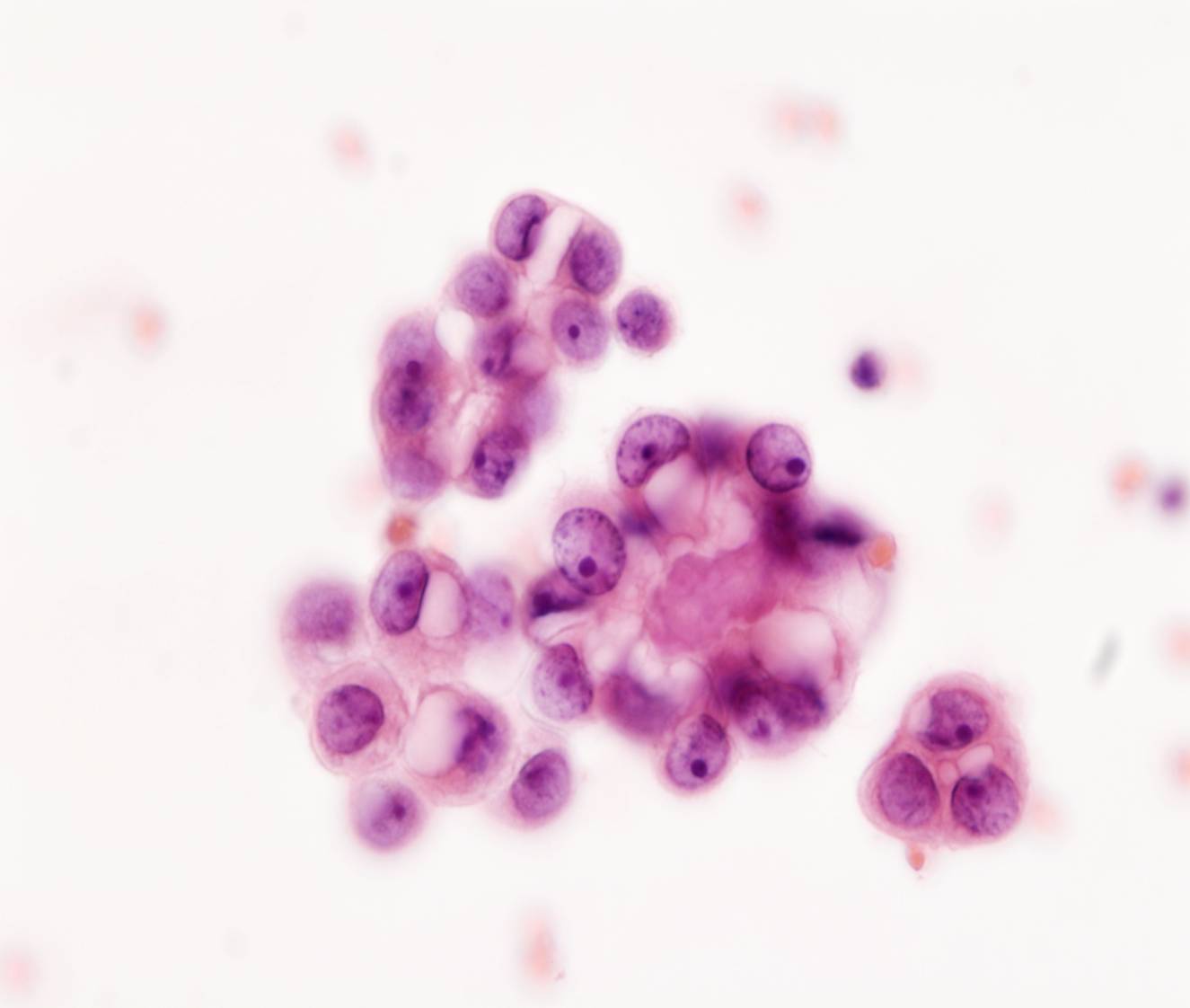
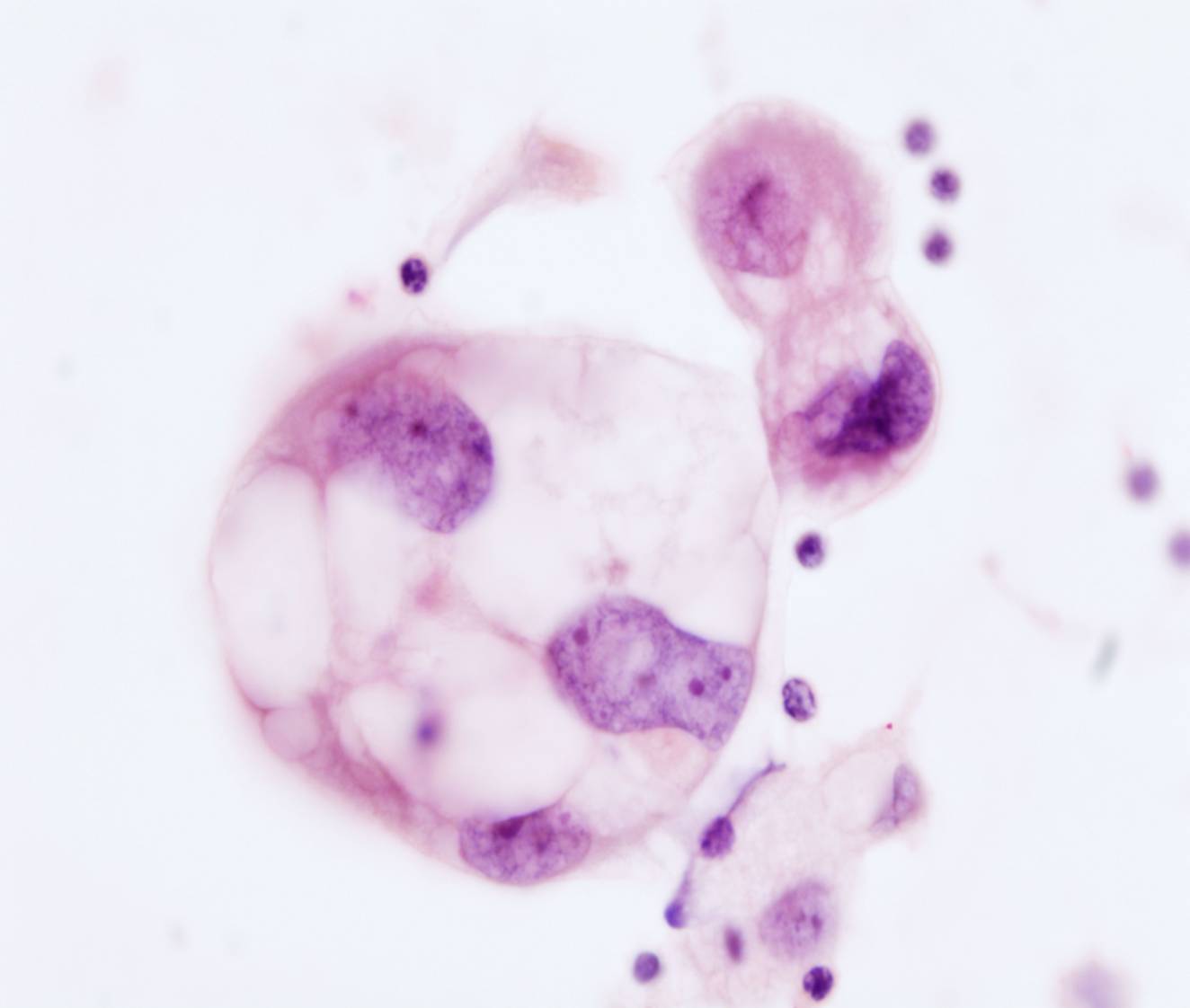
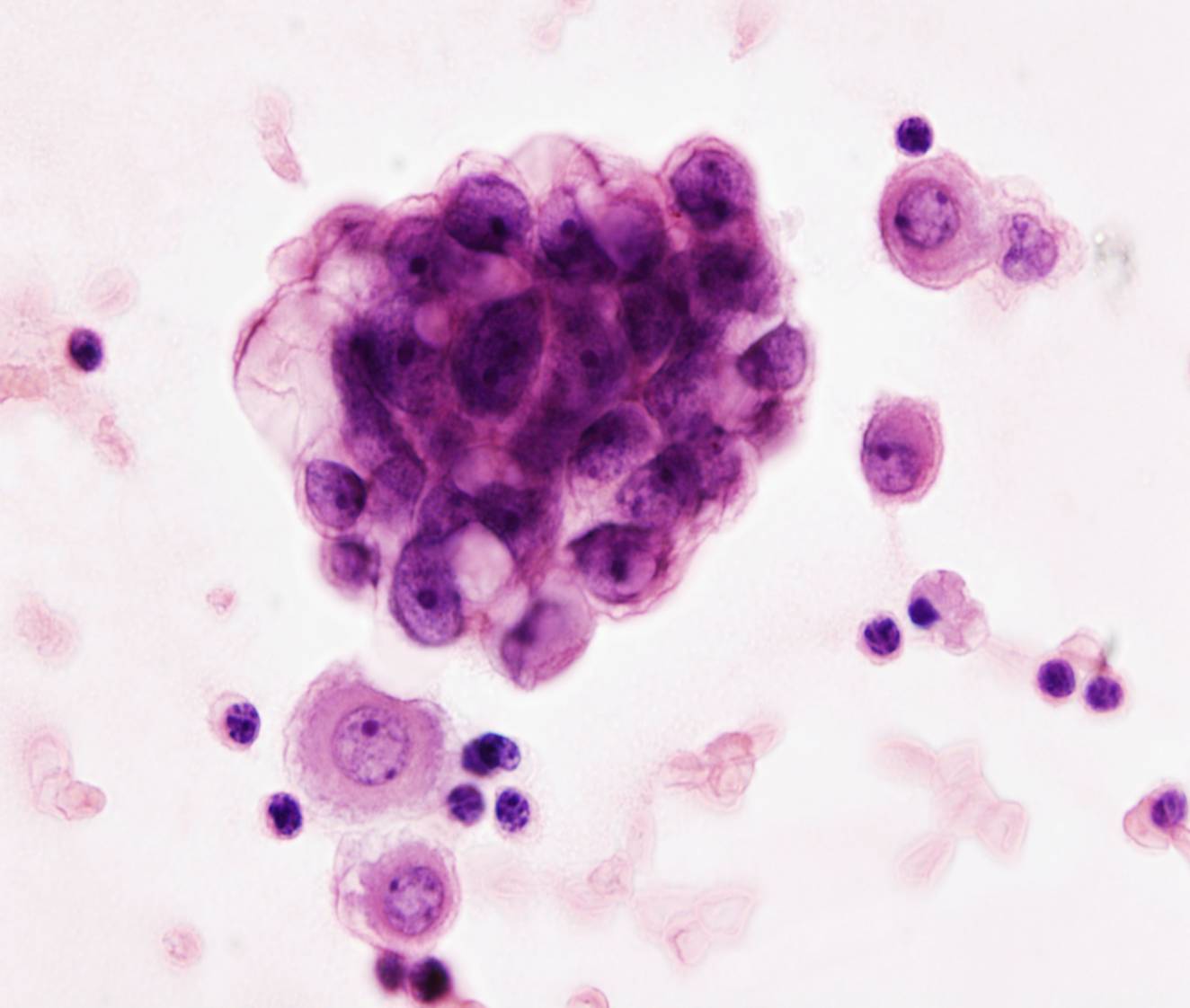
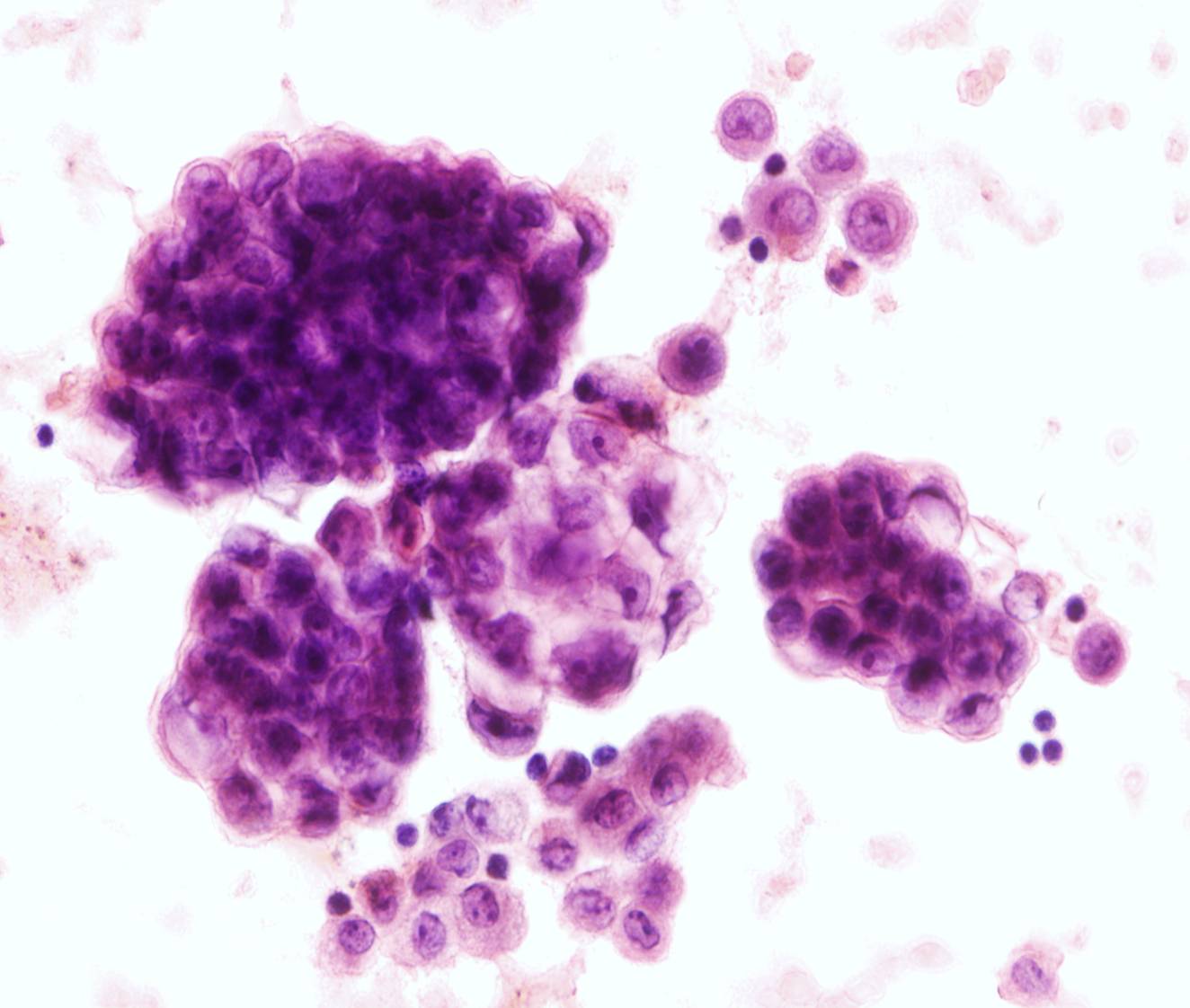
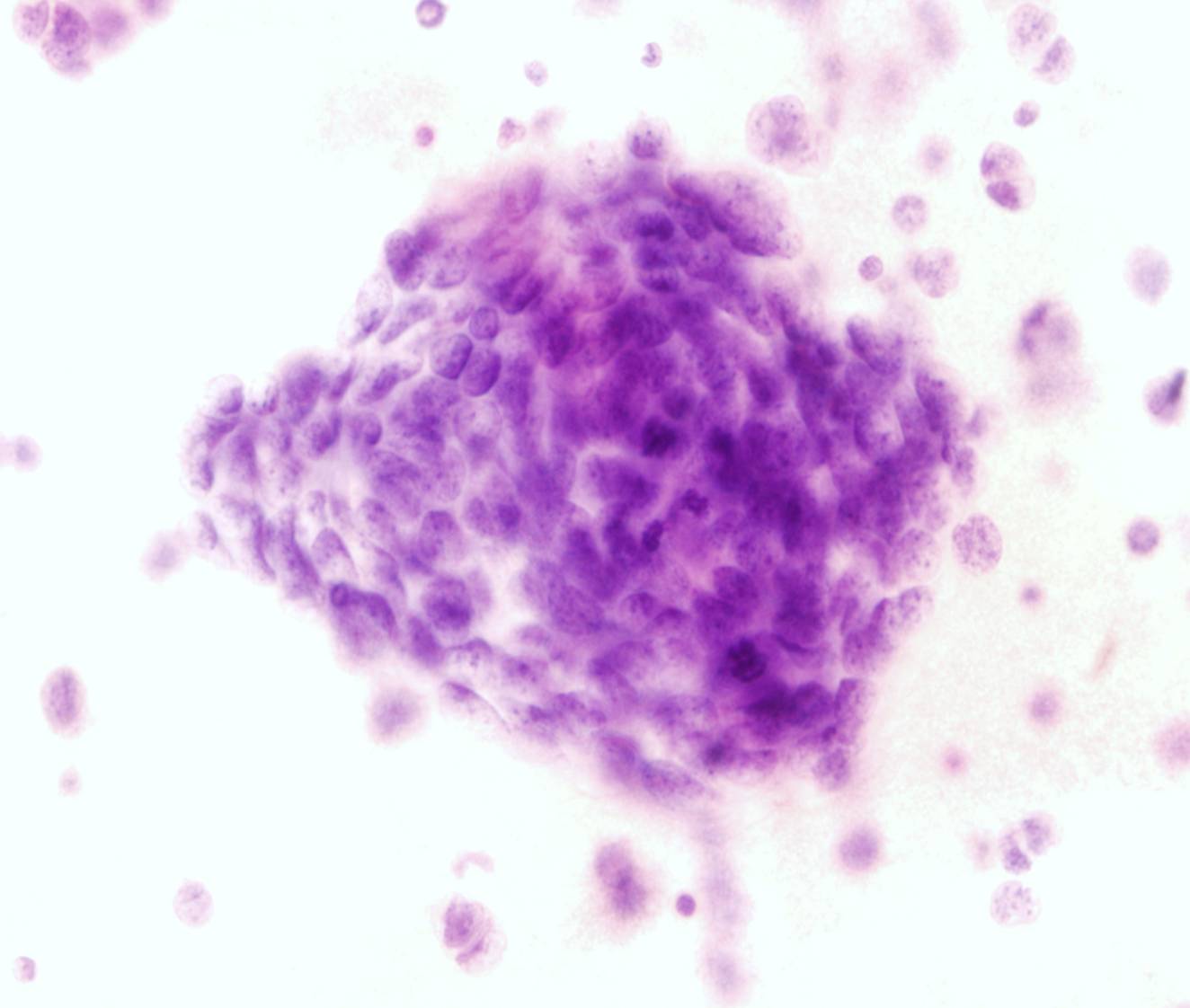
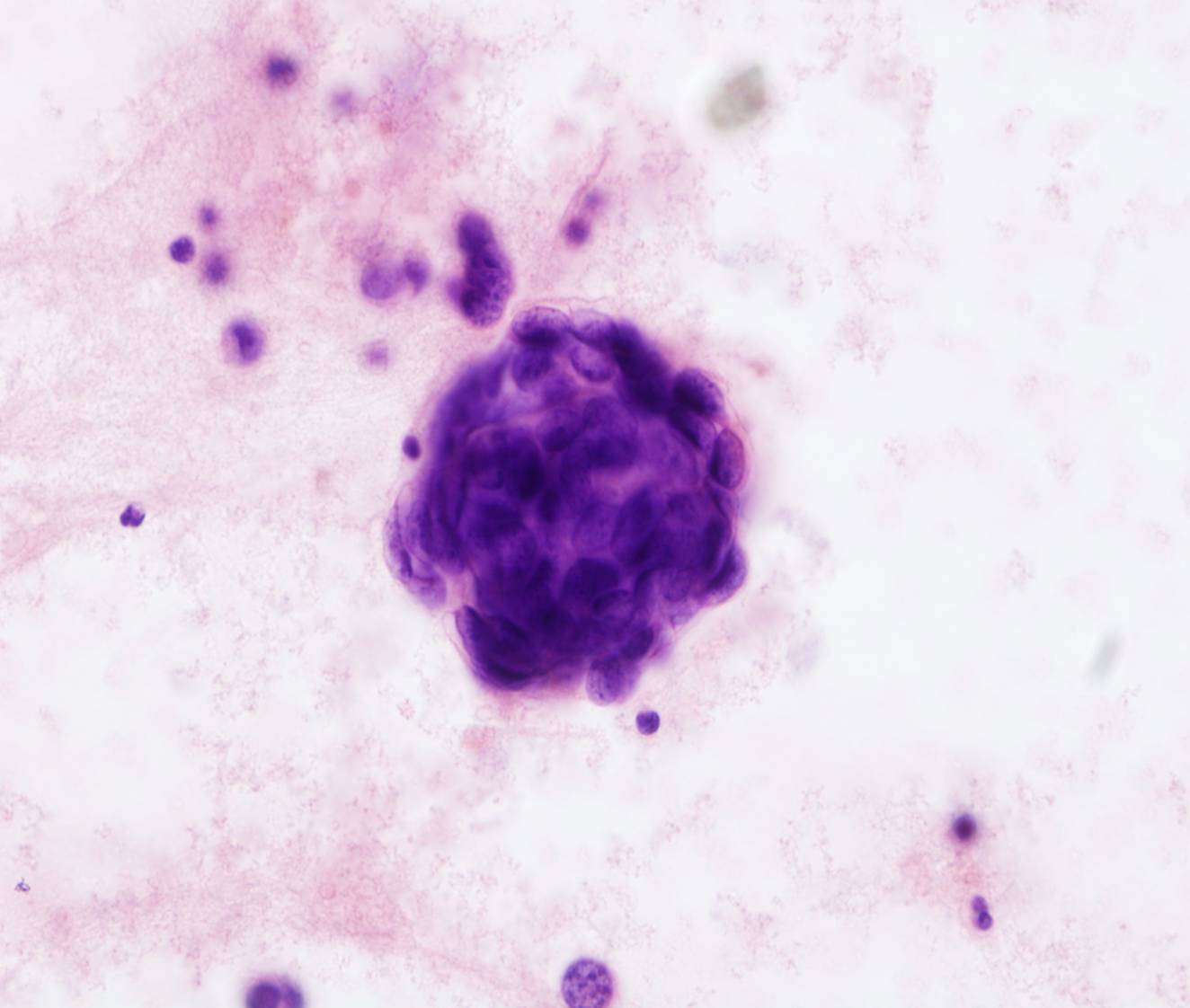
Adenocarcinoma
- Large spheres or single cells
- Cytoplasmic vacuolization
- Signet ring cells (gastric, breast)
Breast, lung, ovary and stomach are the most common primary sites. Some morphologic features can point to the site of origin of an adenocarcinoma. For example, abundant hollow spheres (‘cannonball’) are a common pattern in metastatic breast cancer (ductal carcinoma). Such 'proliferation spheres' may also be present in metastatic ovarian carcinoma as well as in small cell lung carcinoma. Signet ring cells are common in metastatic gastric carcinomas. Most colorectal cancers are composed of elongated cells with hyperchromatic nuclei arranged in acinar formations, often with individual cell necrosis. Large cells with prominent nucleoli and abundant lacy, vacuolated cytoplasm are typical of clear cell carcinomas of the kidney and the female genital tract. Psammoma bodies are observed in effusions caused by serous carcinomas of the ovary, fallopian tube and endometrium, papillary carcinoma of the thyroid, adenocarcinoma of the lung. They are also seen in mesothelioma and in some benign proliferations of the mesothelium. Groups of cells with cytoplasmic vacuolization are typical of metastatic ovarian carcinoma and lung adenocarcinoma. Mucinous tumors, particularly of the ovary and appendix, produce abundant extracellular mucin, which markedly distends the peritoneal cavity (pseudomyxoma peritonei). The fluid is gelatinous and composed predominantly of mucin, which stains blue-green or purple with the Papanicolaou stain. The specimens are often sparsely cellular, containing only vacuolated histiocytes; the tumor cells, columnar and hyperchromatic, are not seen in many cases.
It is usually easy to distinguish malignant cells from reactive mesothelial cells. In block sections malignant cells are often arranged in large clusters or situated in lacunae. In some cases, metastatic adenocarcinoma cells may be hard to recognize, when either a ‘second population’ of benign mesothelial cells is absent or the tumor cells resemble mesothelial cells very closely. Lobular carcinoma of the breast can be particularly difficult to recognize. Special stains for mucin, CEA and Leu-M1 are useful: most adenocarcinomas are positive, whereas mesothelial cells are negative.
Immunohistochemical markers are also useful in patients with tumors of unknown primary.
88 89 90 91
93 94 95 96 97
99 100 102 103
105 106 108 109
111 112 114 115
118 119 120 121
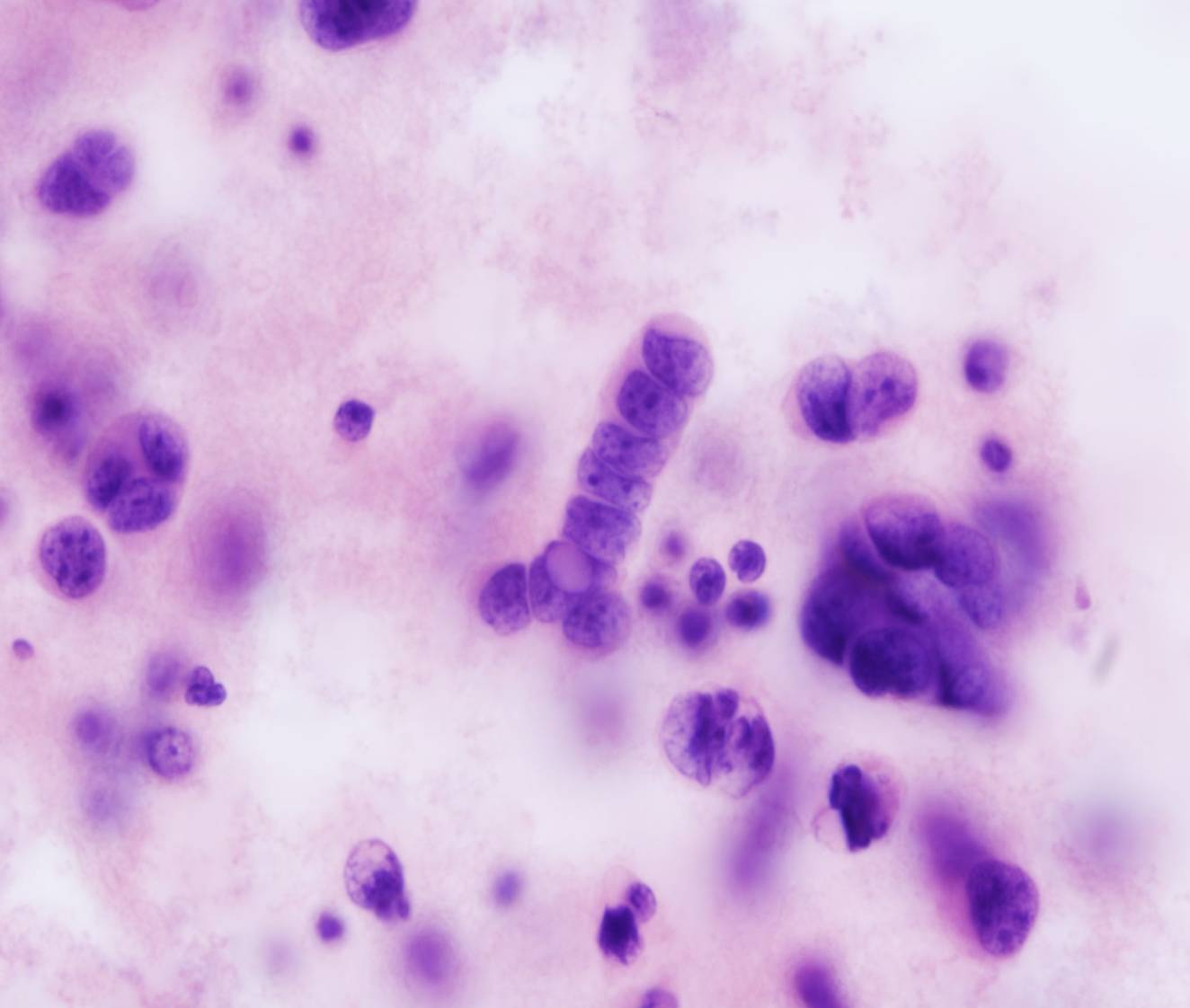
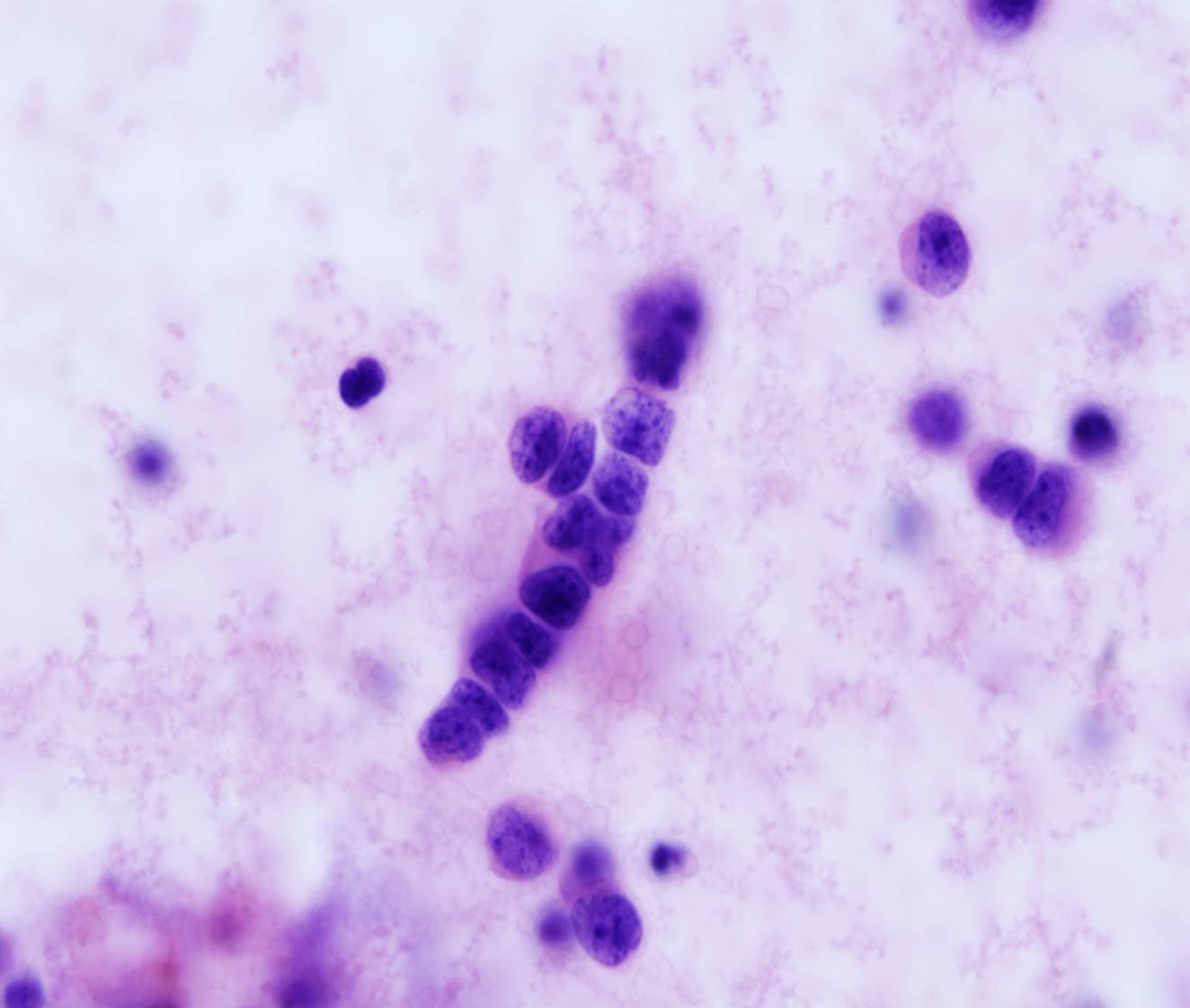
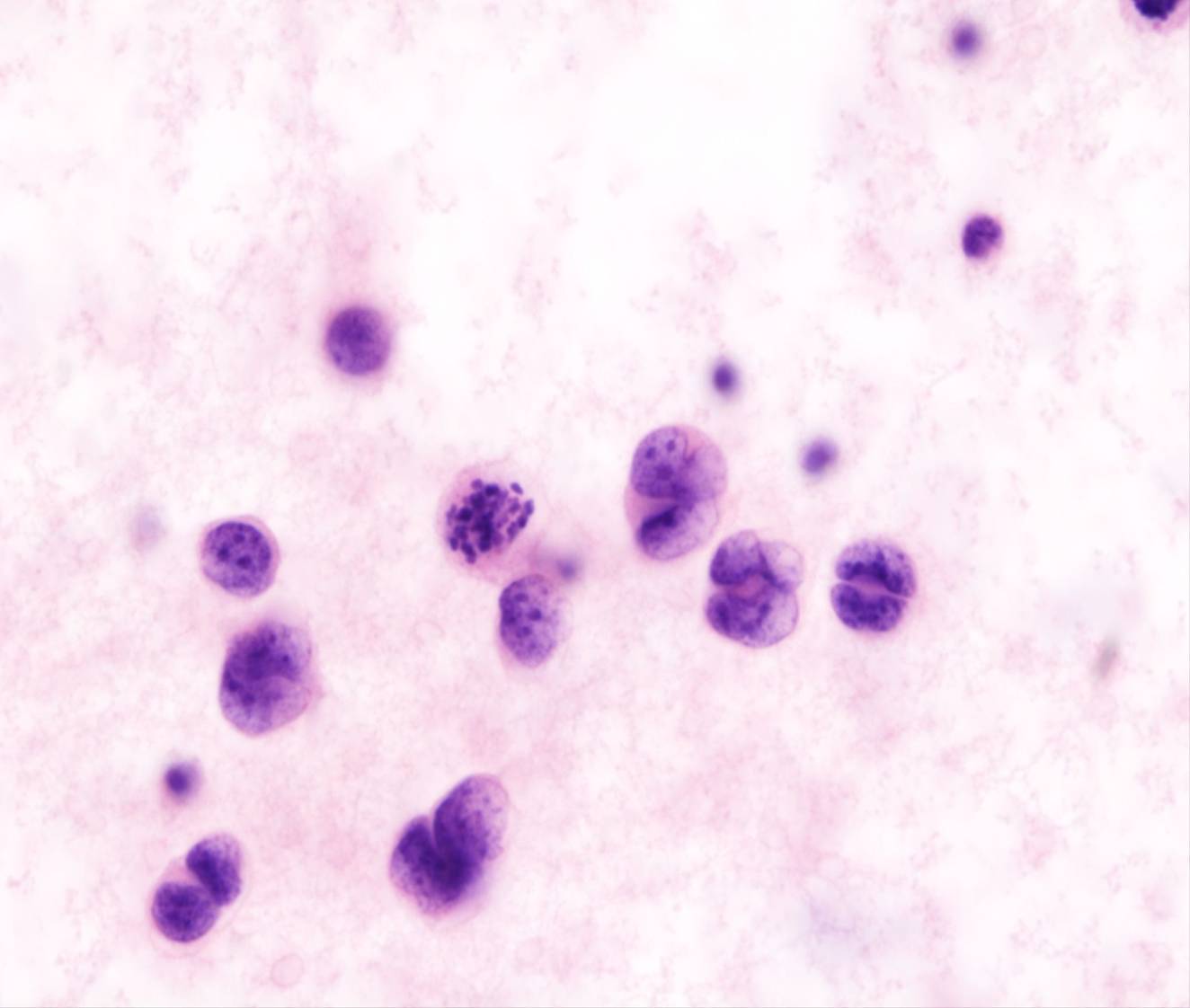
124 Small cell carcinoma
- Isolated cells and cohesive clusters
- Chains of tumor cells with side arms coming off at various angles
- Nuclear molding
- Scanty cytoplasm
- Mitoses
This cytologic appearance is characteristic of small cell carcinomas of the lung as well as of other small cell malignancies (such as Merkel cell carcinoma and neuroblastoma). The cells are small, approximately 2-3 times the diameter of small lymphocytes. The nuclei are dark, with finely granular chromatin texture. The cells of small cell carcinoma are distinguished from those of lymphoma by their tendency to form clusters.
125 126 127 128 129 Squamous cell carcinoma
- Large clusters or isolated cells
- Dense cytoplasm
- Non-keratinizing (mostly) or keratinizing
Squamous cell carcinoma rarely metastatize to the serosal membranes, most commonly from lung, larynx or female genital tract (cervix). The cytologic appearance depends on the degree of differentiation. Nuclei are enlarged and hyperchromatic, nucleoli are usually not prominent. Anucleate squames can be present. Cytoplasmic vacuoles may be present in up to 30% of cases (differential diagnosis with adenocarcinoma)