

A méhnyakrák epidemiologiája, etiológiája, patogenezise és fõbb szövettani típusai
Az invazív méhnyakrák klinikai jellemzése
Az invazív méhnyakrák klinikai megjelenése és a terjedésének jellege igen különbözõ. A daganat lehet polypoid vagy papillomatózus, lehet lapos vagy kifekélyesedõ. Kezdetben a legtöbb rák lokálisan terjed- felfelé a méhtest felé, lefelé a hüvelybe vagy oldalra a kismedence felé. A daganat esetleg beszuri a húgyhólyagot vagy a végbelet és távoli áttéteket ad a májba, és más szervekbe. A betegség korai fázisában már áttéteket adhat a kismedencei nyirokcsomókba ami rossz prognózist jelez.
A méhnyakrákot leggyakrabban 45-65 éves nõkben diagnosztizálják, bár már leírták egészen fiatal nõkben is, így az életkori elõfordulást 20-85 év közé kell tenni. A betegség korai stádiumában a méhnyakrákos nõk gyakran tünetmentesek; korai stádiumban lehet közösülés utáni, intermenstruális vagy menopauza utáni vérzés, hátfájdalom vagy véres vizelés.
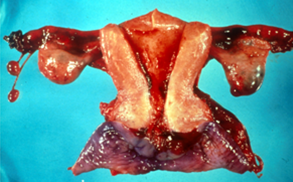 |
| Invaziv cervix rákban eltávolitott méh makroszkópos képe. A cervix kifekélyesedett és daganat infiltrálja. A biopszia fenti diagnozist alátámasztotta. |
Staging invasive cervical cancer
Stage |
FIGO: Description |
| 0 | Preinvasive carcinoma (CIN3 or carcinoma in situ) |
| I | Cervical carcinoma confined to uterus (extension to corpus disregarded) |
| Ia | Invasive carcinoma diagnosed only by microscopy |
| Ia1 | Stromal invasion <3mm depth and <7mm horizontal spread |
| Ia2 | Stromal invasion >3mmbut >5mm and <7mm horizontal spread |
| IB | Clinically visible lesion confined to cervix or microscopic lesion >1A2 |
| IB1 | Clinically visible lesion <4cm in greatest dimension |
| IB2 | Clinically visible lesion >4cm in greatest dimension |
| II | Tumour invades beyond uterus but not to pelvic wall or lower third of vagina |
| IIA | Without parametrial invasion |
| IIB | With parametrial invasion |
| III | Tumour extends to pelvic wall and/or involves lower third of vagina and /or causes hydronephrosis or non functioning kidney |
| IIIA | Tumour involves lower third of vagina but no extension to pelvic wall |
| IIIB | Tumour extends to pelvic wall and /or causes hydronephosis or non functioning kidney |
| IVA | Tumour invades mucosa of bladder or rectum and / or extends beyond true pelvis |
| IVB | Distant metastasis |
Az invazív méhnyakrák kezelése
- . Az invazív méhnyakrák klinikai beosztása fontos, minthogy meghatározza a beteg kezelését. A 0. stádiumban felismert (preinvazív stádiumú) daganatoknál csupán a daganatos, máhrétegen belül elhelyezkedõ terület helyi, diathermiás vagy lézeres sebészi kimetszése szükséges.
- Stage 1 cancers are usually treated by radical hysterectomy with or without preservation of the ovaries according to the patients age.
However in women that have early stage cancer of the cervix, trachelectomy may be used as a fertility saving treatment. A radical trachelectomy is a surgical procedure; whereby the cervix , the upper part of the vagina, the parametrial tissue (tissue around the lower end of the uterus), and the pelvic lymph nodes are removed. The uterus (the womb) and the ovaries are not removed and so it is still possible to have children.
This is done in early cervical cancer; the aim being to preserve fertility. This treatment has been developed in recent years by gynaecological oncologists in specialist centres around the world. It is done vaginally and through small incisions in the abdomen using a laparoscope, (key hole surgery).
- The standard treatments for advanced cervical cancer are radical hysterectomy and/or pelvic radiotherapy.
More advanced cancers may require radiotherapy and /or chemotherapy. The clinical stage at time of diagnosis also affects the prognosis (chances of survival) for the patient.
- The outlook is very good for women with cancer diagnosed in its early stages (Stage 0 or Stage 1) but is poor for women diagnosed with advanced cancer. The prognosis for patients diagnosed at Stage 0 ie the preinvasive stage is excellent with only a very small risk (<less than 1%) of recurrence.
- There is some evidence that cervical cancers in younger women may be more aggressive that those that are diagnosed in women over the age of 40.