| Introduction |
| Technical aspects |
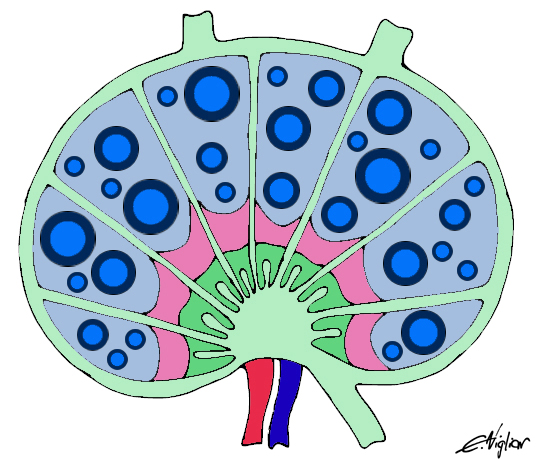
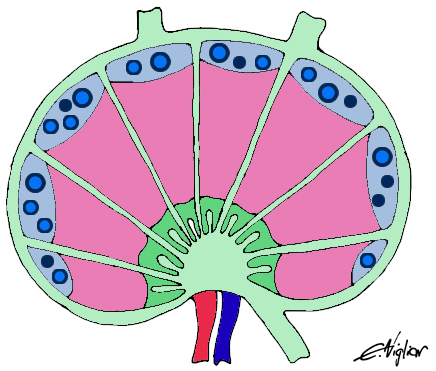
| Normal lymph node histology and cytology |
| Reactive lymph node |
| Hodgkin Lymphoma |
| Non Hodgkin lymphoma |
| Metastases |
REACTIVE LYMPHOADENOPATHY
- General features
- Non-specific hyperplasia
- Viral and post-vaccinial
- HIV infection
- Mononucleosis
- Sinus histiocytosis
- Suppurative lymphadenitis
- Granulomatous lymphadenitis
- Toxoplasmosis
General features
Lymph nodes react to different antigen stimulation with enlargement and expansion of one or all the anatomical areas. The number and sites of the lymph nodes involved as well as the entity and duration of the enlargement are extremely variable. After a recent infection, children may develop significant and persistent lymph node enlargements. Conversely adults generally develop slightly reactive enlargements; hence any lymph node enlargements of adults is often considered suspicious. Ultrasound features combined with Power Doppler are highly sensitive in the identification of reactive lymph nodes; nonetheless FNC is often requested for a diagnosis, to avoid surgical biopsies. Cytological features may display lymphoid, granulomatous or suppurative patterns but the cytological features are unspecific in most cases.
Back to topNon-specific hyperplasia
FNC of most of lymph node enlargements shows a variable mixture of normal cell type constituents. Vascular structures and phagocyting histiocytes may be present, conferring a polymorphous appearance to the smear. When a lymphadenopathy is determined by the expansion of the follicular centres, the smears show numerous centrocytes and centroblasts intermingled with small mature lymphocytes, plasma cells and immunoblasts. In cases of interfollicular expansion the smears show a prevalence of mature lymphocytes, plasma cells and immunoblasts; epithelioid cells may also be present. In both cases, more monomorphous smears pose the problem of the differential diagnosis with NHL. FC and PCR may help in differential diagnosis. In immunodeficy syndromes and autoimmune diseases FC may occasional show light chains restrictions in a small percentage of the cells. In these cases, as well as in all doubtful cases, histological control should be performed.
Differential diagnosis: follicular lymphoma (see NHL).
Back to topNon-specific hyperplasia with follicular centre expansion
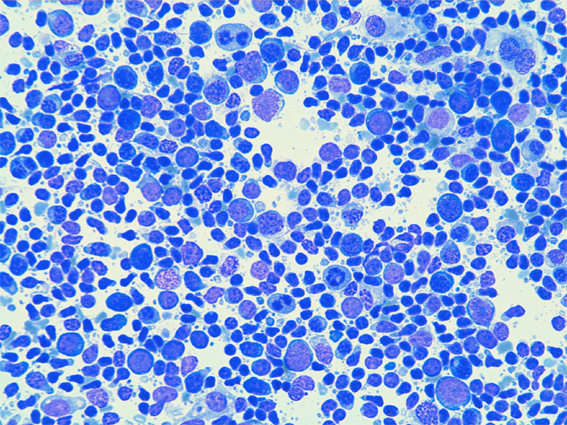
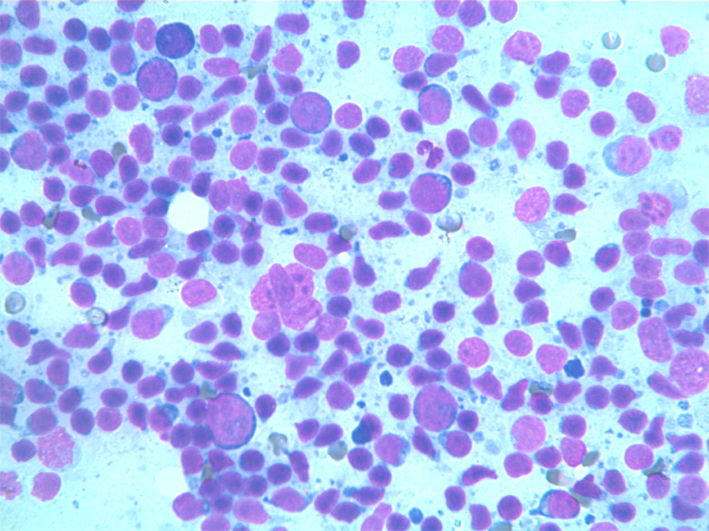
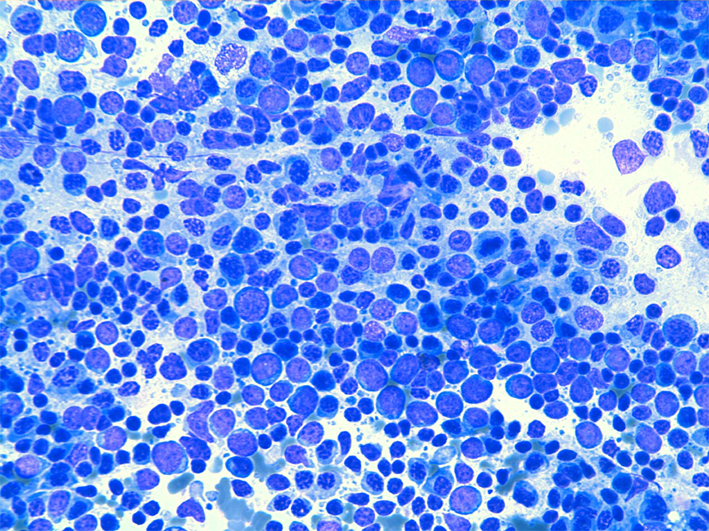
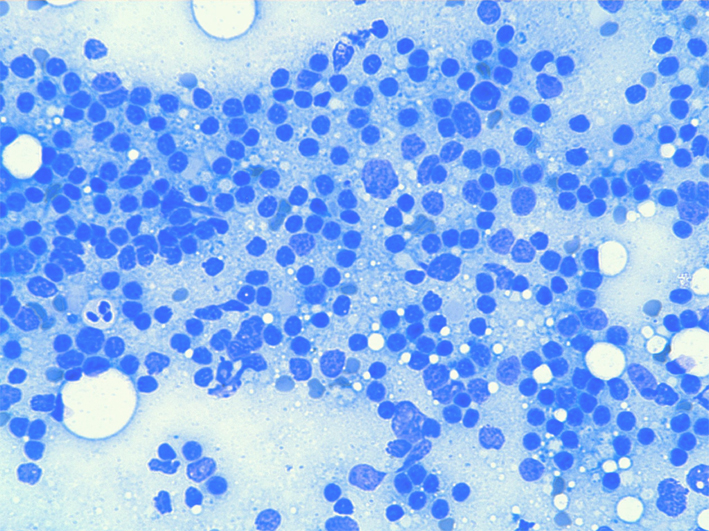
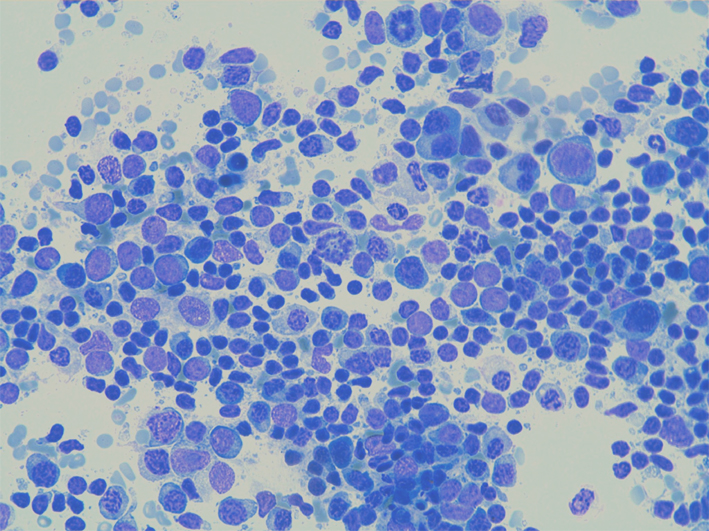
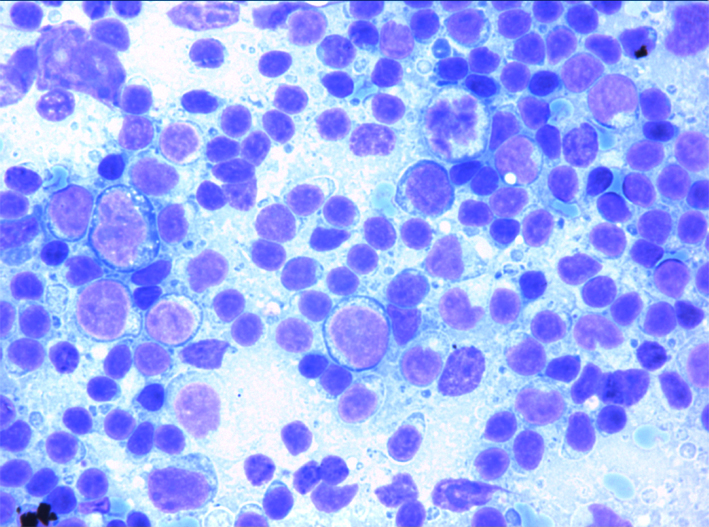
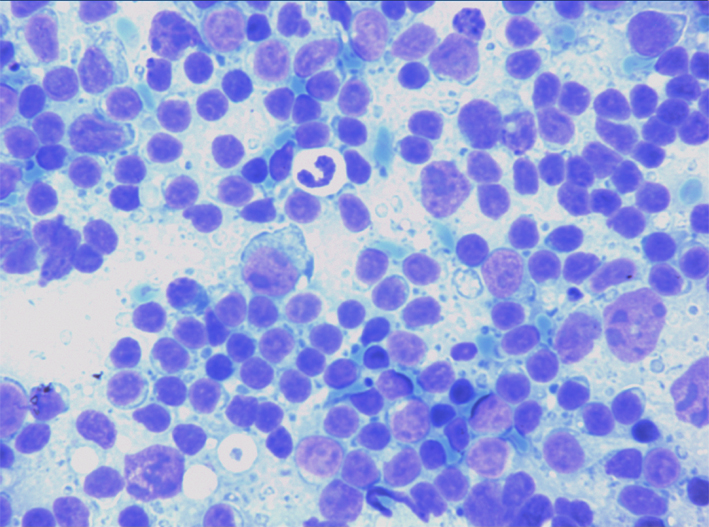
Non-specific hyperplasia with follicular centre expansion: smears show numerous centrocytes and centroblasts with two or more eccentrical nucleoli intermingled with small mature lymphocytes with slightly lengthened nuclei and cytoplasmic tales, plasma cells and immunoblasts.
Non-specific hyperplasia with follicular centre expansion: smears show centrocytes and centroblasts; these latter have two or more eccentrical nucleoli. lymphoid bodies, small mature lymphocytes with slightly lengthened nuclei and cytoplasmic tales are also present.
Relatively monomorphous, non-specific hyperplasia with follicular centre cells and mature lymphocytes. Differential diagnosis with a possible low-grade non Hodgkin lymphoma is often impossible without ancillary techniques.
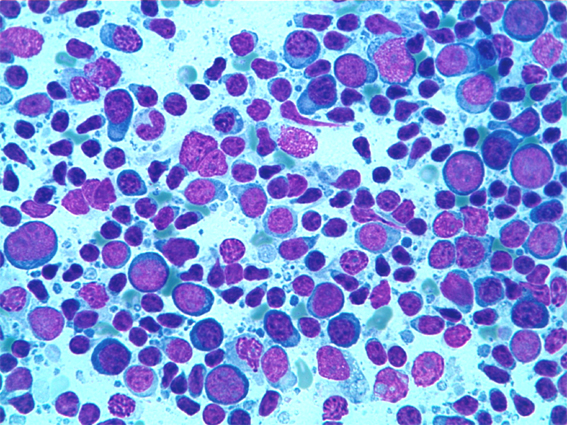
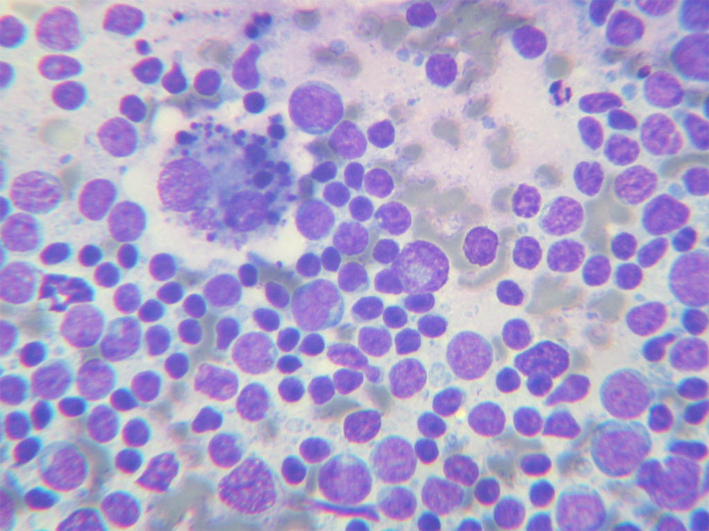
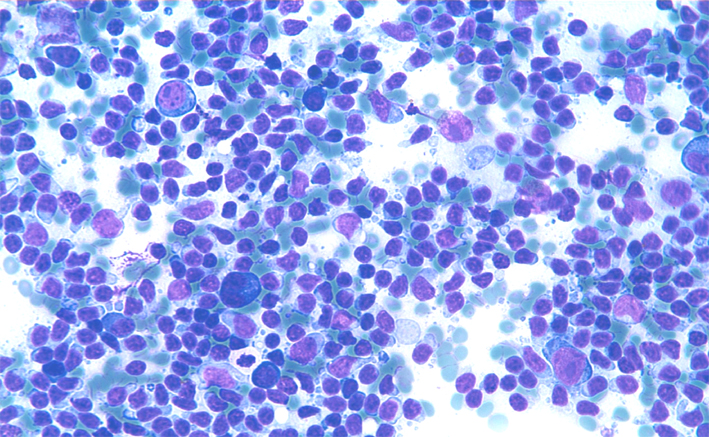
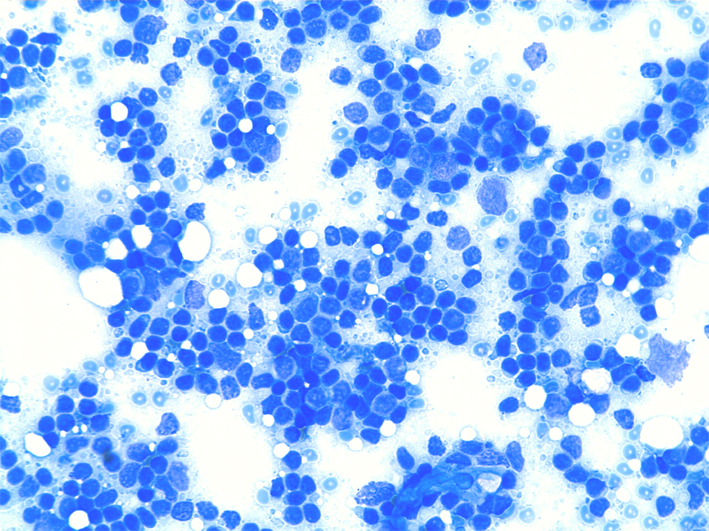
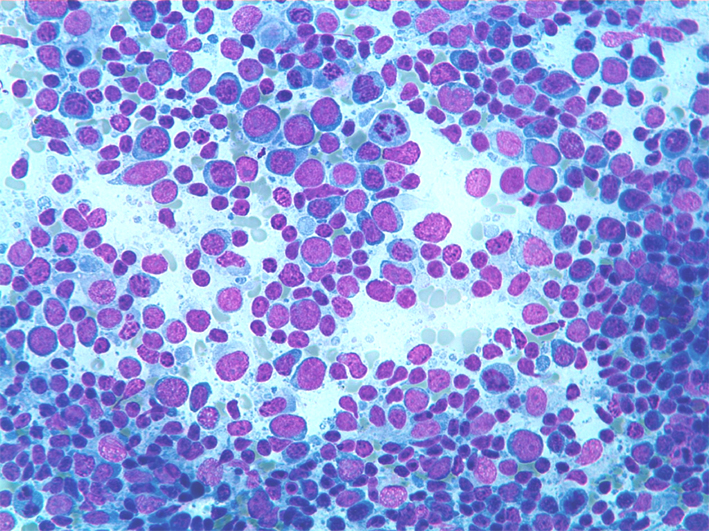
Non-specific hyperplasia with follicular centre expansion: smears show numerous centrocytes and centroblasts with two or more eccentrically located nucleoli intermingled with small mature lymphocytes. Macrophages with large cytoplasm engulfed with nuclear debris are generally present.
Non-specific hyperplasia with numerous plasma cells in a polymorphous background. Plasma cells may be observed in a spectrum of reactive lymphadenopaties including reumatoid, luetic and dilantin lymphadenopaties; Castleman disease may also show an excessive number of plasma cells. A polymorphous cytological smear and a polyclonal phenotype should be sufficient to exclude a possible lymphoplasmacytic lymphoma.
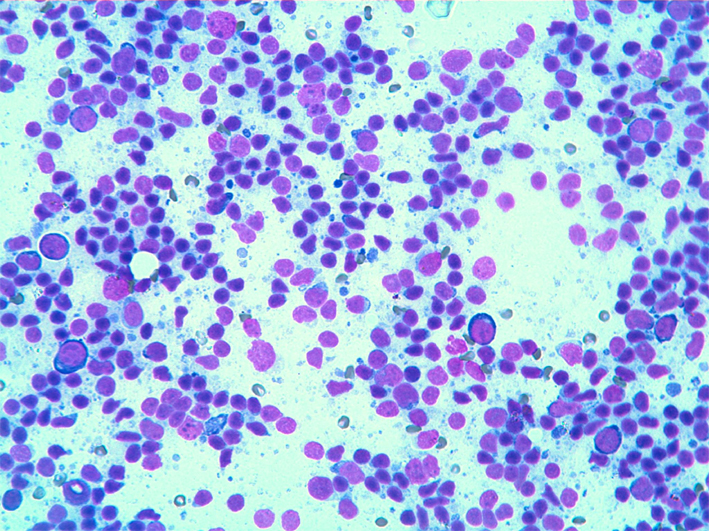
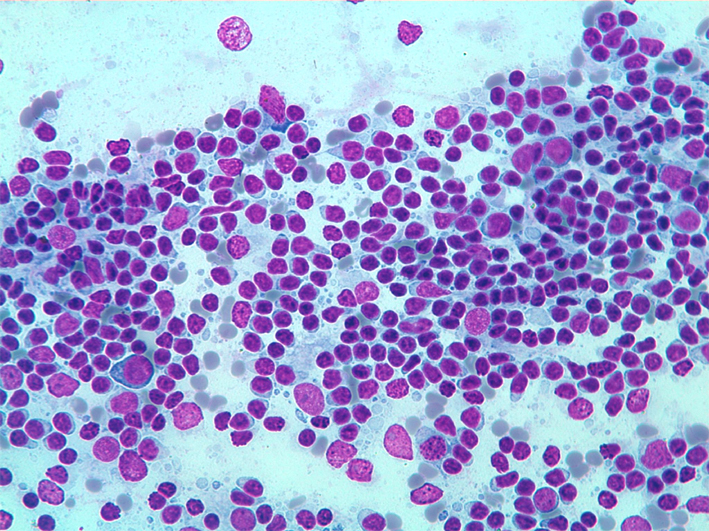
Non-specific hyperplasia with follicular centre expansion: smear show numerous follicular centre cells and small mature lymphocytes. Vascular structures are often present, even with branching appearance, with small lymphocytes tightly attached.
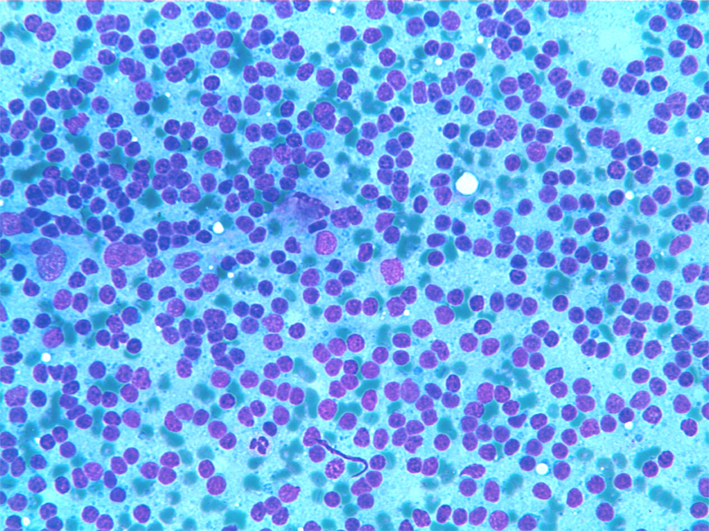
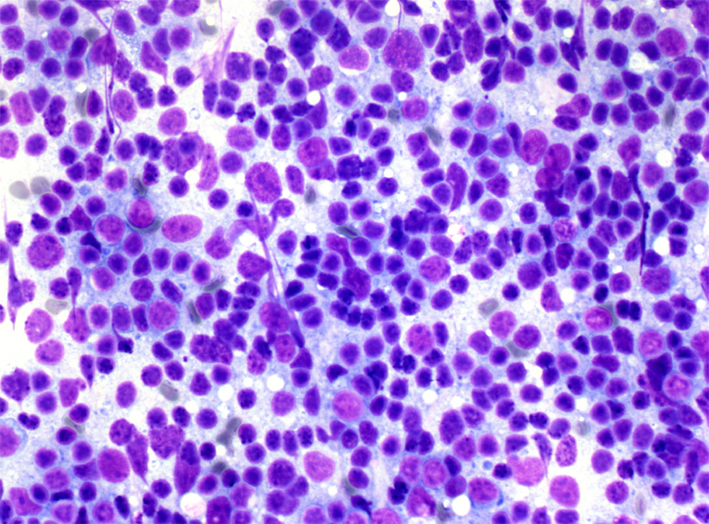
Non-specific hyperplasia with follicular centre expansions smears show numerous centrocytes and centroblasts intermingled with a variable number of small lymphocytes. Differential diagnosis with a NHL is often pointed out.
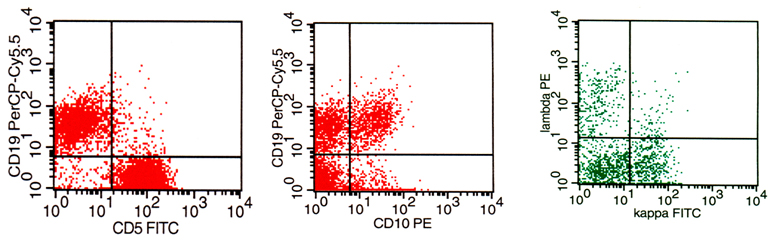
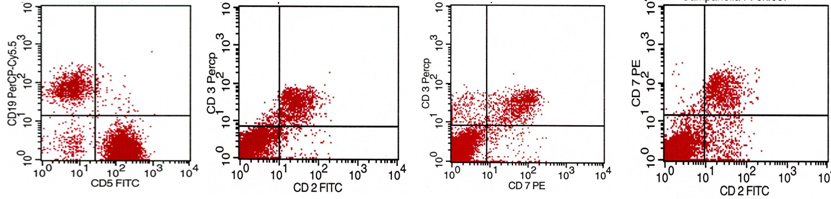
Flow Cytometry of non-specific hyperplasia with follicular centre expansions: histograms show T and B-cell populations (a), a follicular centre cell population which co-expresses CD19/CD10 (b) and balanced expression of kappa and lambda light chains (c).
Back to topNon-specific hyperplasia with interfollicular expansion
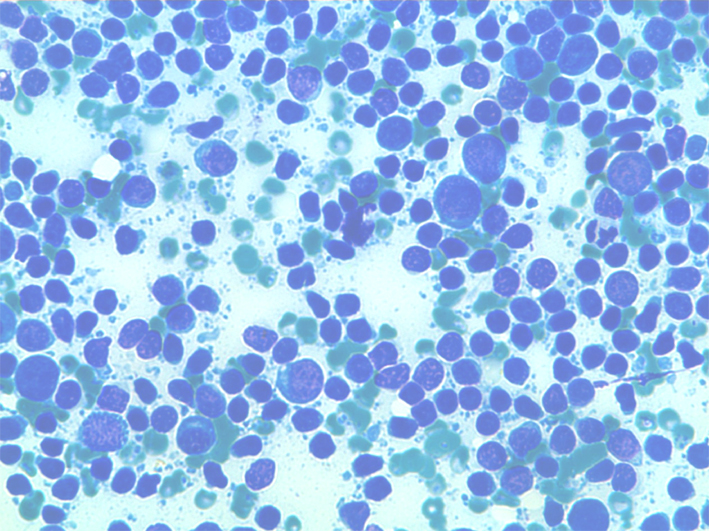
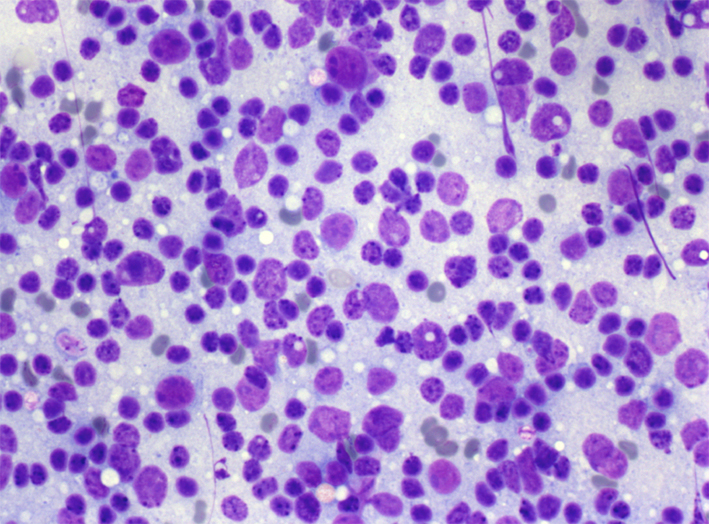
Non specific hyperplasia with interfollicular expansion: the smear shows a prevalence of mature lymphocytes with large nucleolated immunoblasts and plasma cells.
Non specific hyperplasia with inter-follicular expansion: the smears may be monomorphous showing a prevalence of mature lymphocytes and occasional immunoblasts. These cases may be indistinguishable from small cell NHL and require phenotypization for diagnosis.
Flow Cytometry in non specific hyperplasia with interfollicular expansion may shows a prevalence of T-lymphocytes (CD5) with CD2/3/7 co-expression.
Back to topViral and post-vaccinial
FNC show small lymphocytes and numerous centrocytes and centroblasts intermingled with small mature lymphocytes, plasma cells and immunoblasts. Capillary structures, phagocyting histiocytes and eosinophils may also be present. Differential diagnosis: follicular lymphoma (see NHL).
FNC show small lymphocytes and numerous centrocytes and centroblasts intermingled with small mature lymphocytes, plasma cells and immunoblasts. Numerous mitoses may be present.
Back to topHIV infection
The cytological pattern may vary, ranging from suppurative to granulomatous or non-specific. In case of florid follicular hyperplasia the smear shows numerous centrocytes and centroblasts intermingled with small mature lymphocytes and plasma cells. Differential diagnosis: follicular lymphoma (see NHL).
Numerous centrofollicular cells intermingled with small mature lymphocytes in a lymph nodal reactive hyperplasia in a HIV patient.
Back to topMononucleosis
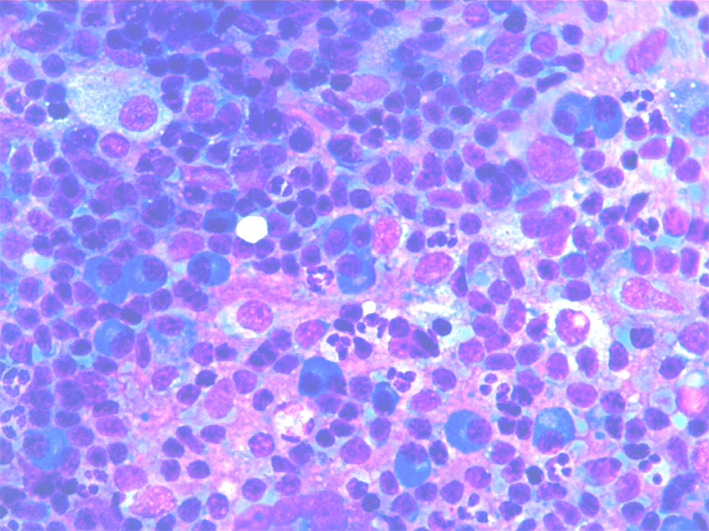
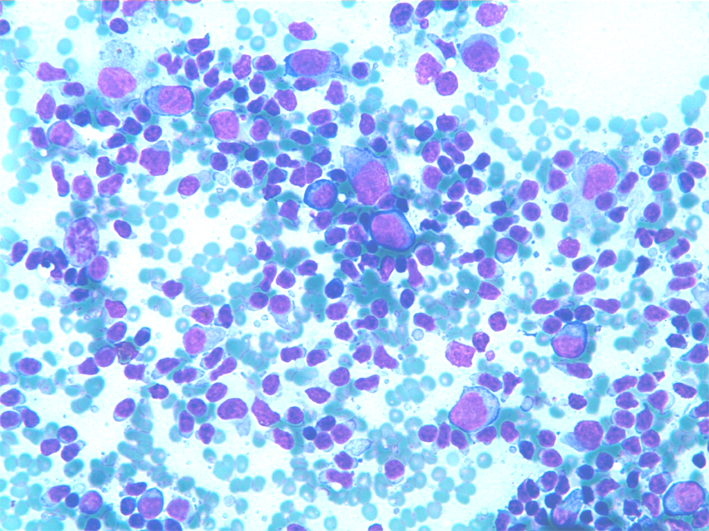
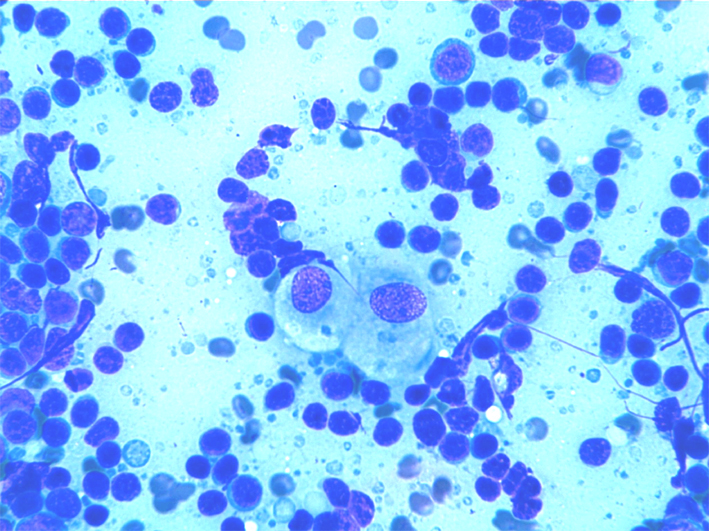
FNC shows normal cell type constituents including centrocytes and centroblasts. Numerous immunoblasts with large nucleoli and a rim of blue cytoplasm are present. Macrophages and capillary structures may be present.
Differential diagnosis: Hodgkin lymphoma (see HL).
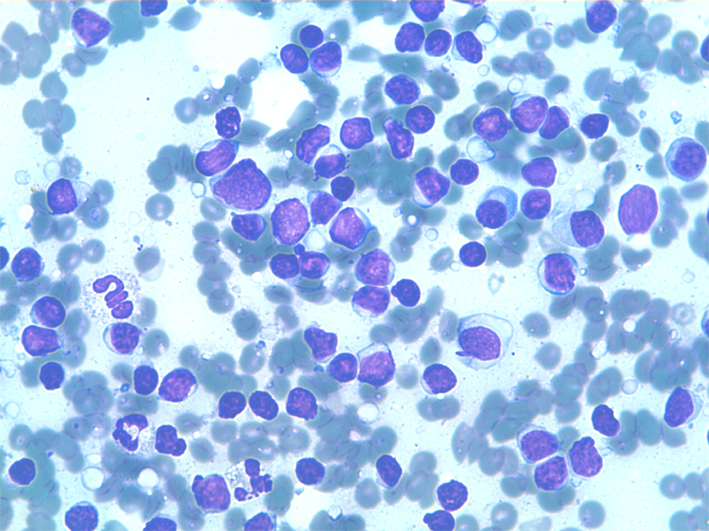
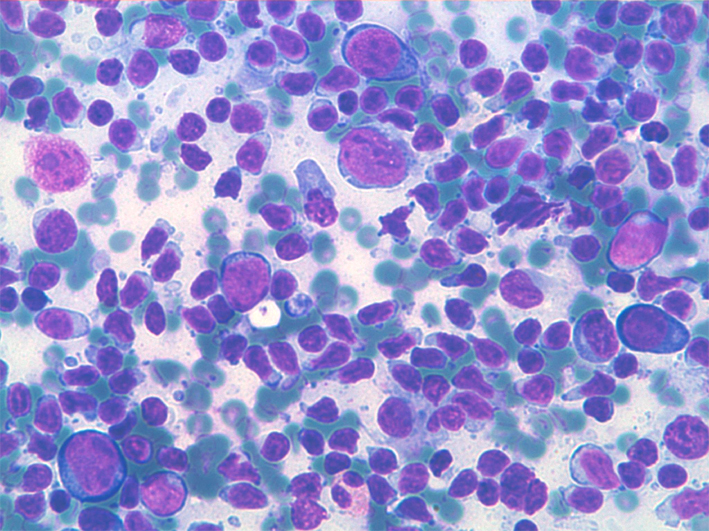
Numerous immunoblasts with large nucleoli and a rim of blue cytoplasm and small lymphocytes in the background.
Immunoblasts with two or three very large nucleoli and a rim of blue cytoplasm; mitoses may be obseved.
Back to topHistiocytosis
This is mainly observed in lymph nodes draining inflamed tissues or organs or cancer. Corresponding smears may show histiocytes, small lymphocytes and macrophages with engulfed cytoplasm.
Differential diagnosis: Sinus histiocytosis with massive lymphadenopathy.
Sinus hysticytosis: smear show mono and multinucleated macrophages often engulfed with nuclear debris in a necrotic and inflamatory background.
Back to topSuppurative lymphadenitis
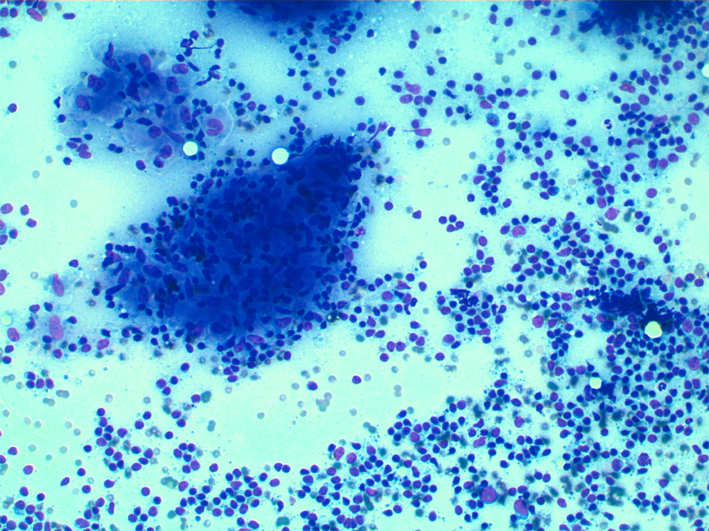
This condition can be observed in lymph nodes draining bacterial infections. Smears show of granulocytes and a variable amount of lymphocytes in a necrotic background. Attention should be paid because metastatic squamous cell carcinoma and rarely HL, may show a prevalent necrotico-suppurative background.
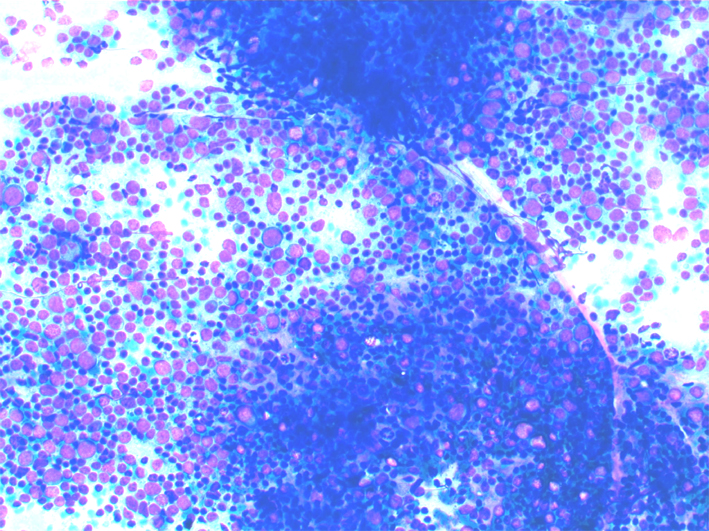
Suppurative adenitis smears show granulocytes occasional histiocytes and few lymphoid cells in a necrotic background.
Back to topGranulomatous lymphadenitis
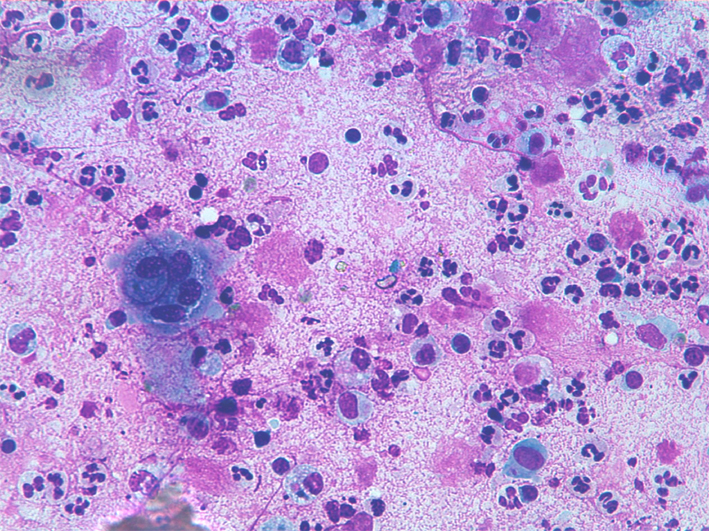
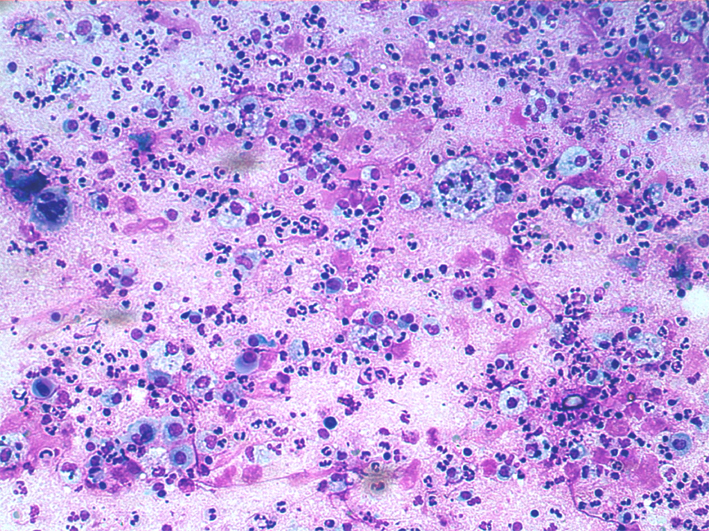
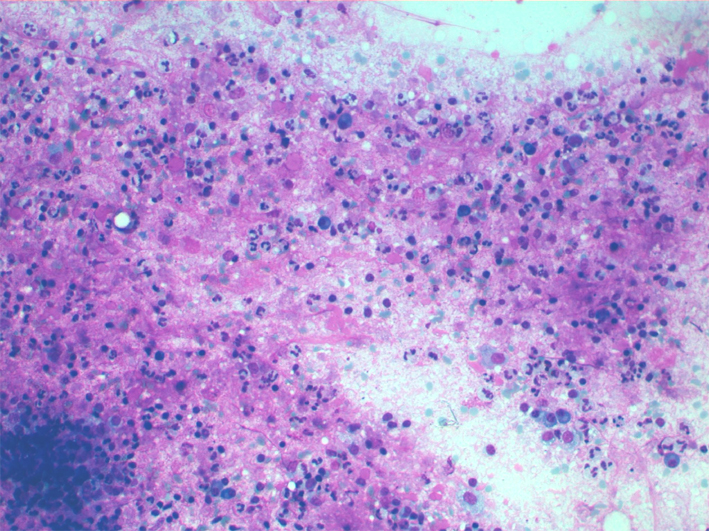
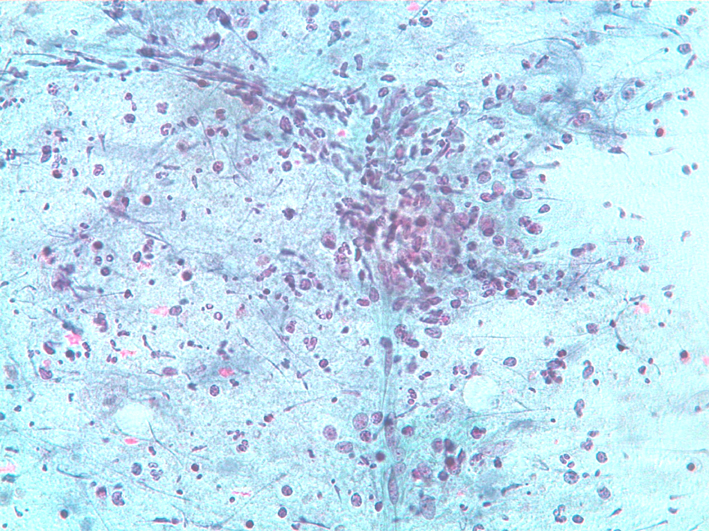
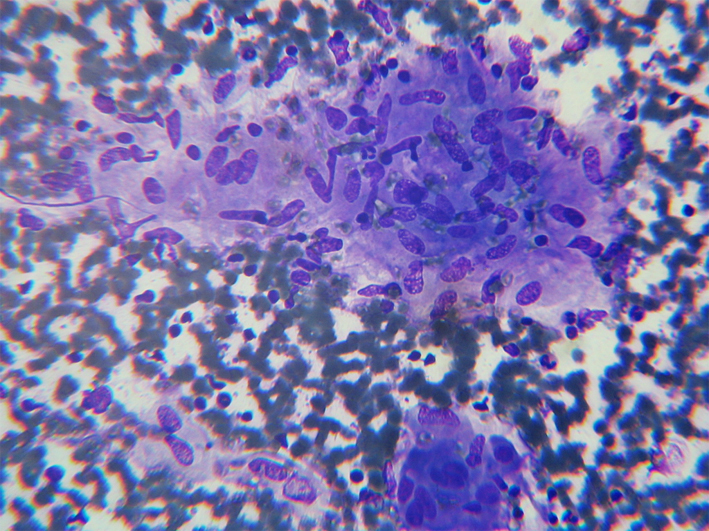
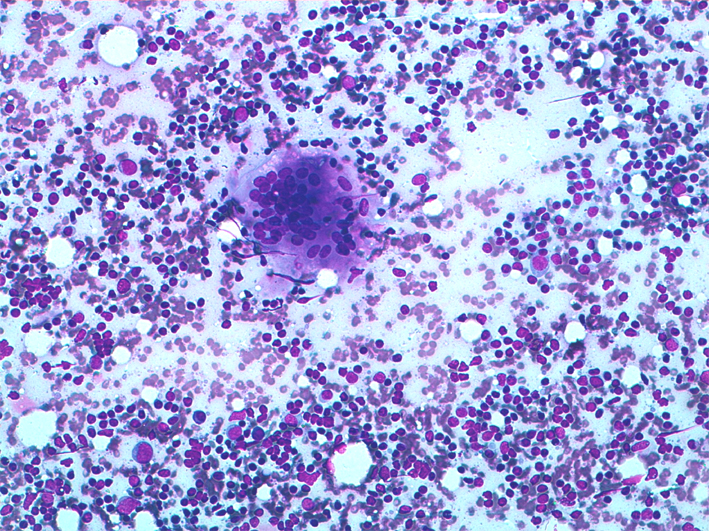
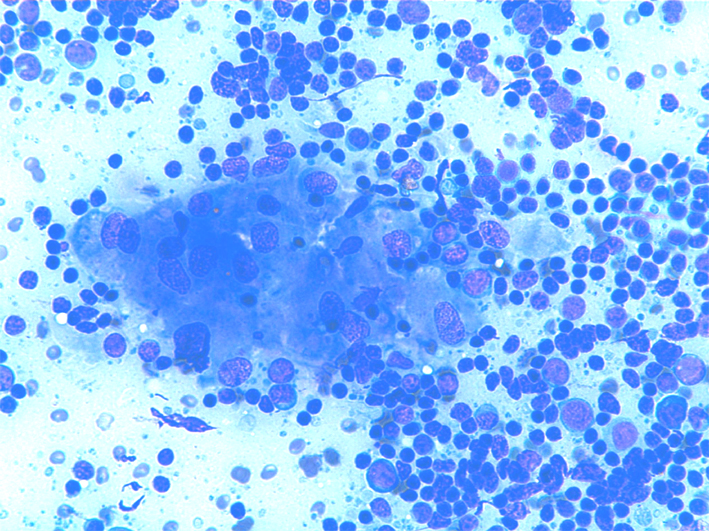
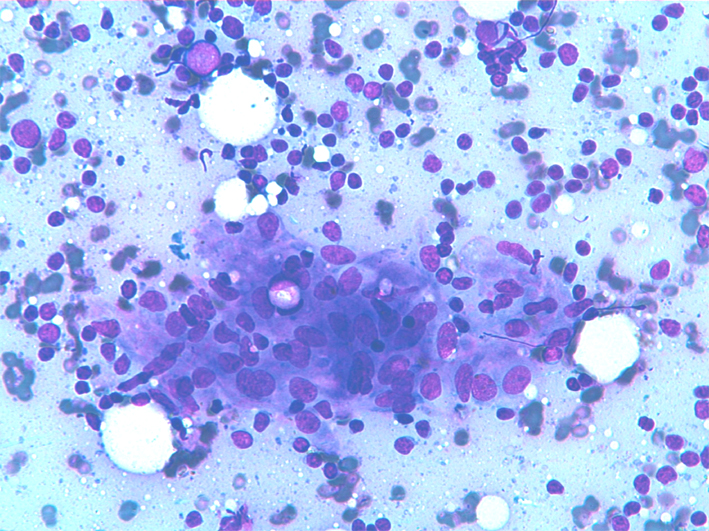
Granulomatous lymphadenitis may be determined by several infective agents or determined by different pathological processes, sarcoidosis and tuberculosis being the most frequent. Granulomatous lymphadenitis may also occur along hematological diseases or after chemotherapy or radiotherapy. Smears show epithelioid cells and/or multinucleated giant cells, either isolated or in a granulomatous arrangement in a lymphoid background.
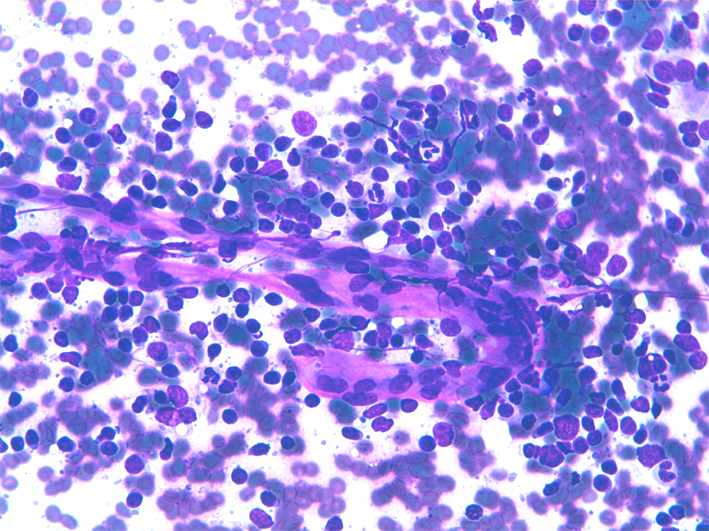
Granuloma showing oval or elongated nuclei in a syncytial cytoplasm
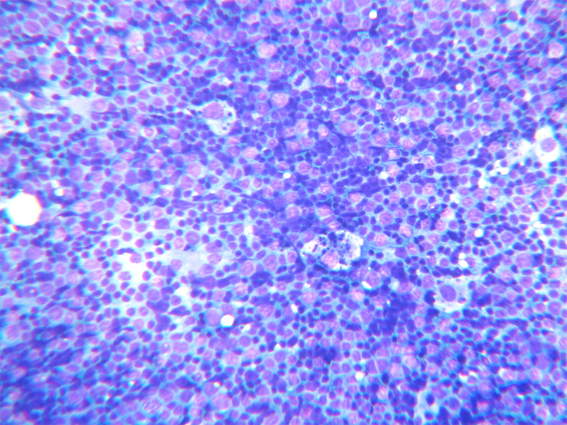
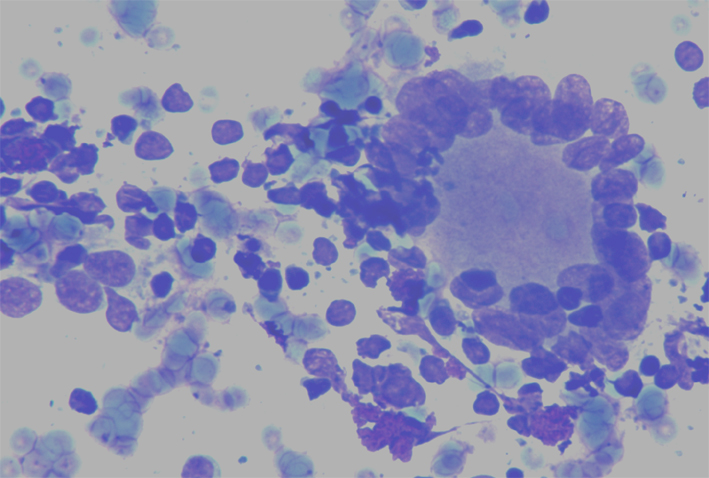
Epithelioid cells organized in granulomas in a lymphoid background
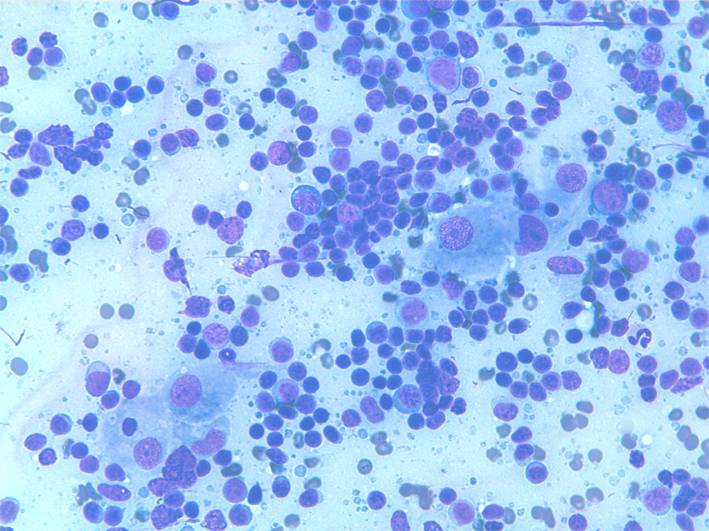
Different cytological patterns in granulomatous lymphadenitis: epitheliod cells organized in small granulomatous striuctures and multinucleate giant cells are intermingled with mature lymphocytes. Note a multinucleated giant cell Langhans type.
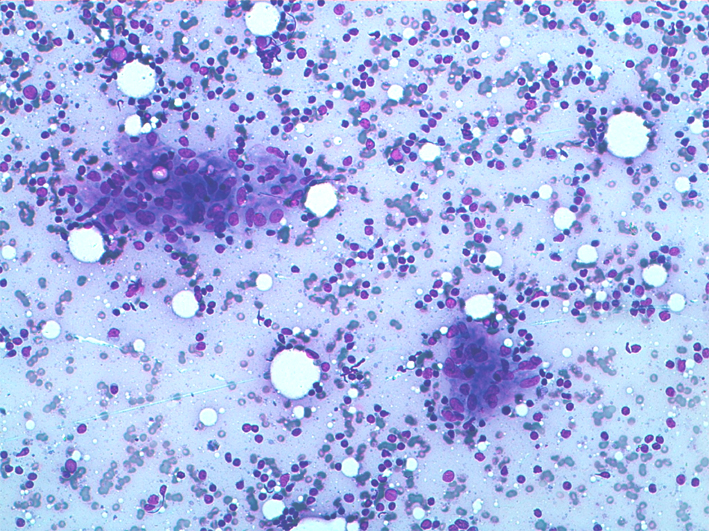
Toxoplasmosis
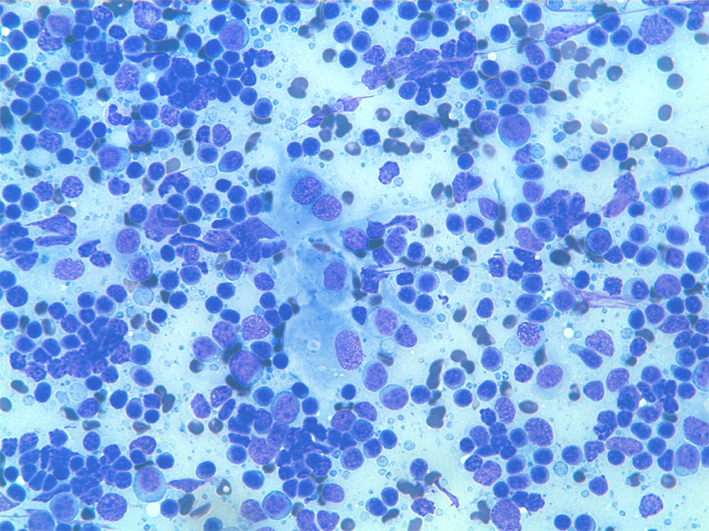
Toxoplasmosis reactive lymph node: small groups and isolated epitheliod cells intermingled with lymphocytes.
Toxoplasmosis reactive lymph node: isolated and grouped epitheliod cells intermingled with lymphocytes. Isolated epitheliod cells show nuclear debris within cytoplasmic vacuoles.
Back to top