Negative (benign) aspirate
This category accounts for the vast majority of FNA aspirates, proportions from different series ranging from 50-75%. Between 60-85% of negative aspirates are obtained from either dominant nodules within nodular hyperplasia or dominant nodules of non-toxic goitre. The remainder of negative specimens are obtained from other benign lesions, such as cysts, inflammatory lesions (e.g. thyroiditis), or clearly identifiable adenomas (although most cytopathologists group all adenomas as suspicious).
As the sensitivity of thyroid FNA is high, the majority of nodules with negative FNA results do not warrant surgical excision. A negative FNA however is not conclusive evidence of the absence of malignancy, particularly as FNA has a false-negative rate of between 1 and 11%. If clinical suspicion persists, further investigation and/or surgical excision is recommended. It is also current practice that even benign nodules with little/no clinical suspicion are followed up, often with further FNAs before the patient is discharged.
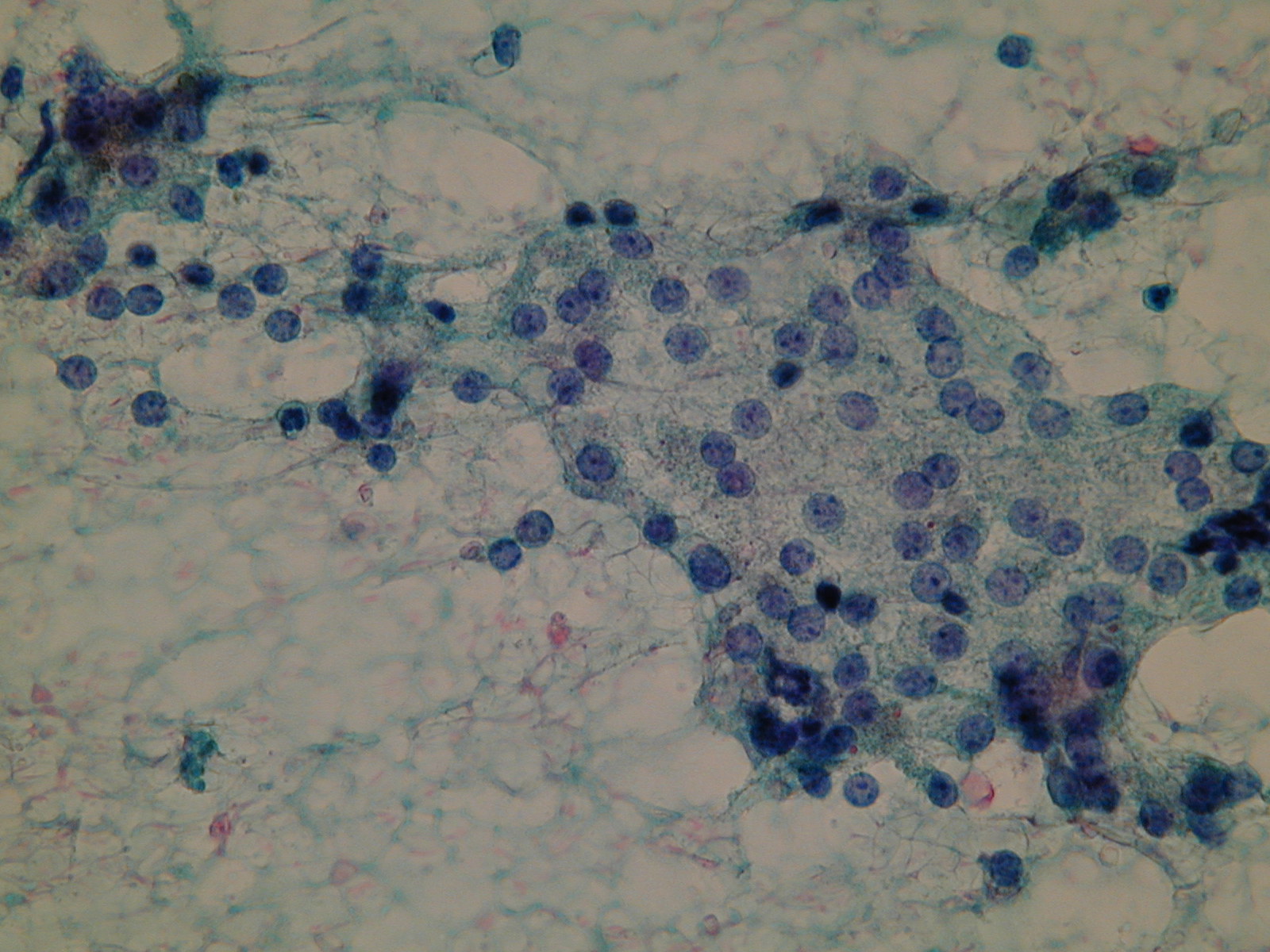
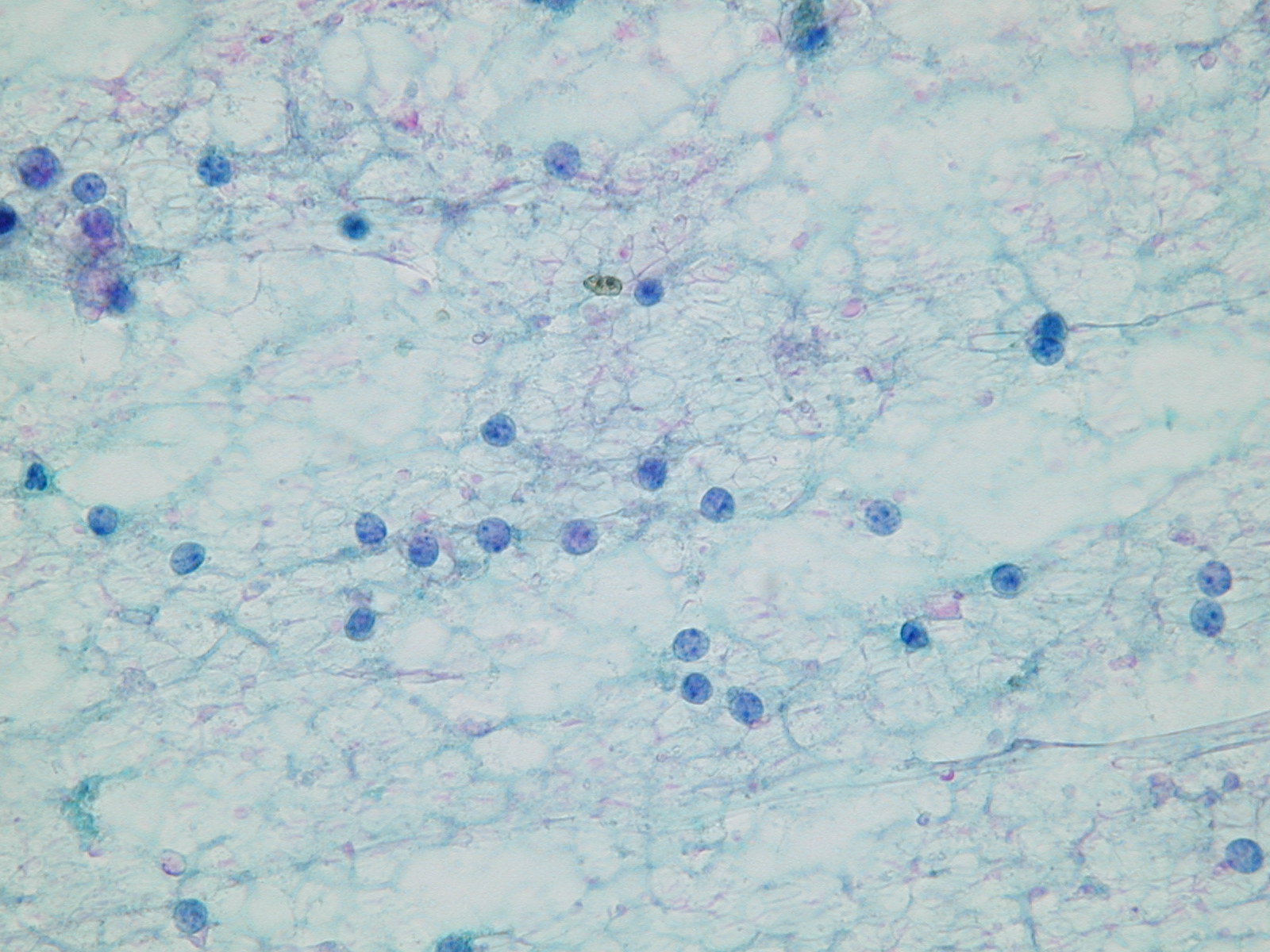
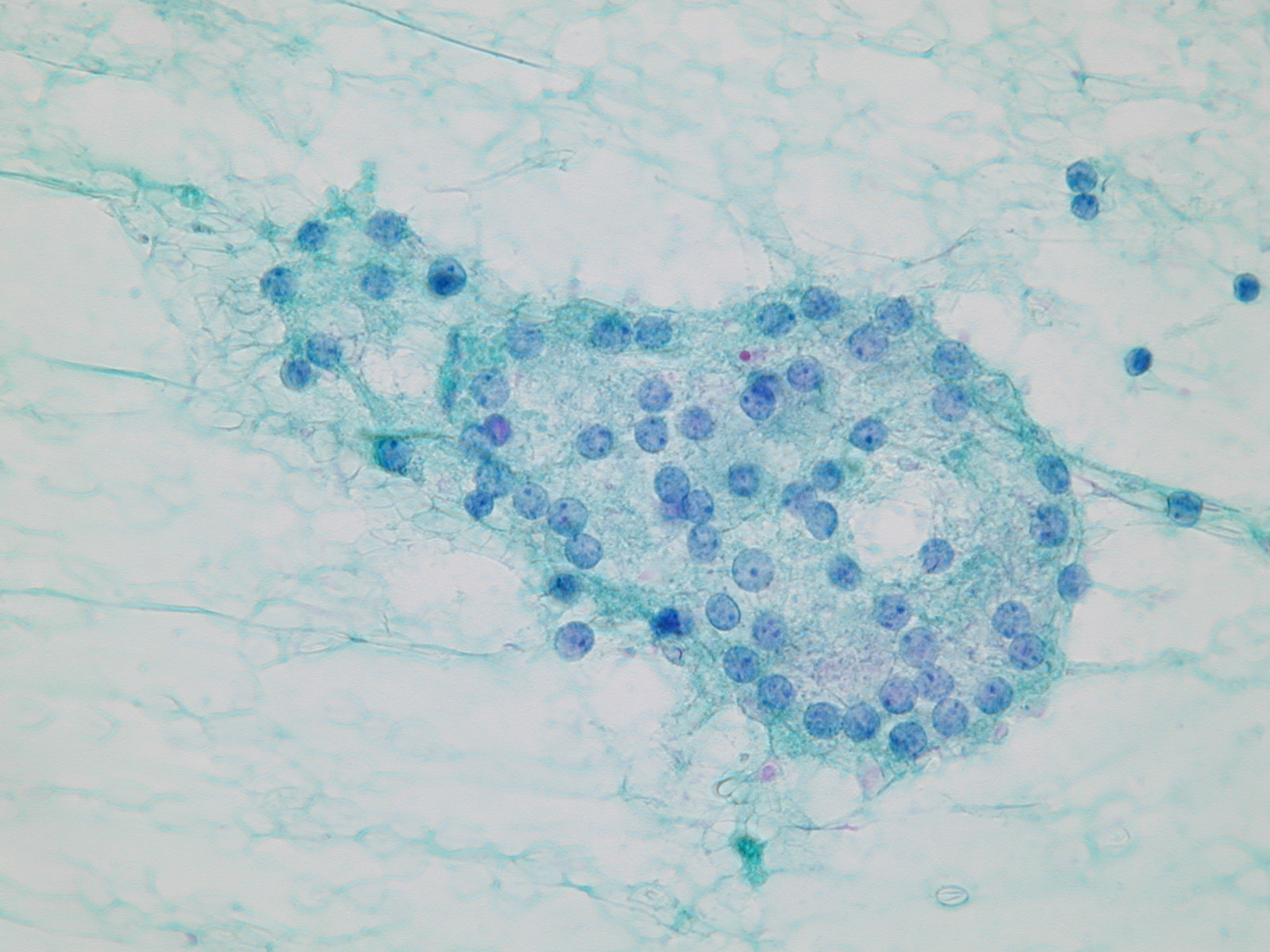
Bland thyroid cells and few bare nuclei. Bare nuclei. Bland thyroid cells in a follicular arrangement.