

Cervical cancer: Epidemiology, aetiology, pathogenesis and main histological types
Histological features of CIN
- Structural changes in epithelium
- Replacement of whole thickness of cervical squamous epithelium with abnormal epithelium
- Undifferentiated abnormal cells with high N/C ratio replace basal layers with loss of polarity. The level at which these undifferentiated cells are found determines grade of CIN.
- Abnormal maturation and abnormal stratification of epithelium
- Increased cellularity of epithelium
- Cellular changes in epithelium
- Presence of mitoses- often abnormal
- Nuclear pleomorphism, variation in size and shape
- Hyperchromasia
 |
 |
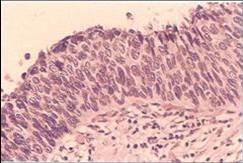 |
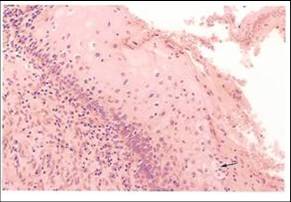
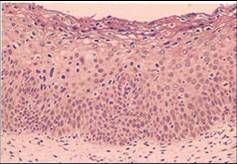
| CIN1 : note undifferentiated abnormal cells with high n/c ratio occupying the lower 1/3 of the epithelium and abnormal maturation with loss of stratification in the upper 2/3 of the epithelium. | CIN2: note abnormal cells with high n/c ratio occupying 2/3 of the epithelium,showing loss of polarity and presence of mitotic figure .Some abnormal maturation is seen in upper 1/3 of epithelium | CIN3: note abnormal cells with high n/c ratio occupy full thickness of epithelium. They show loss of polarity, pleomorphism, hyperchromasia and mitotic figures |
Cervical Intraepithelial Neoplasia may progress to invasive cancer if not treated
- Risk of progression increases with grade of CIN
- Highest risk of progression with CIN3, lowest with CIN1
- May remain stationary
- Progression may take up to 20 years
- CIN1 may regress
- No sharp boundaries between CIN1/2/3
Evidence to support that untreated CIN may lead to invasive cancer
- Indirect evidence that CIN 1, 2, and 3 are a lesional continuum is based on experimental studies. Direct evidence that CIN is a precursor of invasive cancer was obtained by prospective studies of women with untreated CIN . A brief review of these studies is presented below.
- Experimental studies which support the concept of CIN1,2,and 3 as a lesional continuum
- Autoradiographic studies of the proliferative activity of normal cervical epithelium , dysplasia and carcinoma in situ .These were carried out by Richart (1963) who labelled DNA synthesising cells in cervical biopsies with tritiated thymidine . He found that the regeneration time of the epithelium decreases with the severity of the cervical lesion and was least in carcinoma in situ .
- DNA cytophotometric studies of biopsies of normal and dysplastic epithelium and carcinoma insitu . Willbanks et al (1967) measured the DNA content of the cells in Feulgen stained sections using a microspectrophotometric method and showed that the DNA content increased with increasing severity of the cervical lesion and the degree of deviation of DNA values from normal was greatest in carcinoma in situ.
- Studies of cervical carcinogenesis in animals In these studies the cervices of mice were painted with a carcinogenic substance (3,4-benzpyrene) twice a week (Rubio and Lagerhof (1974) .They found that changes consistent with mild dysplasia developed in the cervical epithelium of the mice after two months, moderate dysplasia after four month and severe dysplasia, carcinoma in situ and microinvasive cancer after five months.
- Other interesting experimental work included cytogenetic studies (Spriggs et al 1971); ultrastuctural studies (Murphy et al 1975) and tissue culture studies of cancer cells (Richart 1964).
- Prospective studies of women with CIN
- Evidence to support the concept that CIN is a precursor of invasive cancer has been obtained from prospective studies of women with dysplasia who were not treated but were kept under cytological and /or colposcopic observation over varying periods of time . Although the studies are considered ethically unacceptable today, they provide unequivocal evidence that untreated dysplasia can progress to carcinoma in situ and invasive cancer over time . They have also shown that some dysplasias regress. Many of the studies involved small number of women who were followed over a short period of time and the conclusions based on their outcomes are insecure.
- Arguably, the most convincing survey is that carried out by Mc Indoe et al from New Zealand where women with carcinoma in situ were routinely followed up by cytology on the assumption that the risk of progression was very low (Green and Donovan 1970, Green 1974). Prospective follow up showed that the risk of invasive cancer after an initial diagnosis of carcinoma in situ was very high in women who were managed in this way . Eighteen percent (18%) of the women developed invasive cancer after 10 years and 36% after 20 years.
- The studies described above demonstrate convincingly that untreated CIN lesions can progress to invasive cancer. However , they also show that CIN can regress to normal. This observation has implications for the management of women with CIN. Because in the studies cited above , the gradings of individual lesions at a particular point in time are not known it is difficult to be absolutely sure at which stage the chances of regression of the CIN lesion is greater than the risk of progression . Clinicians tend to agree that the chance of mild dysplasia(CIN1) regressing to normal is high (30%) and are prepared to adopt a "wait and see" policy (at least for 6 months) before determining treatment when CIN1 is diagnosed cytologically
Author |
Study Group |
Outcome |
Fox 1967 |
278 women with mild dysplasia followed for 11 years without biopsy |
Lesion regressed to normal in 31% , |
Richart & Barron |
557 women with dysplasia |
Rate of progression of all degrees of dysplasia to carcinoma in situ was 80% |
Kinlen and Spriggs 1978
|
Traced 52 British women with abnormal smears (Pap class IV or V) who did not attend for treatment for at least 5.2 years after the abnormal smear report |
Repeat smear was normal in 37% |
Nasiell et al (1986) |
555 women with mild dysplasia followed without biopsy for 12 years |
Lesion regressed in 62% |
Mc Indoe et al (1984) |
948 women with biopsy proven carcinoma in situ followed by cytology only from 5 to 28 years |
22% of 131 women who continued to have abnormal cytology developed invasive cancer |