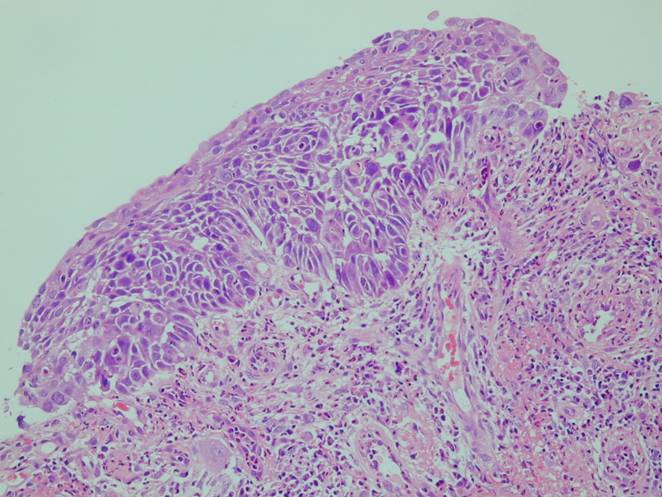
Squamous cell carcinoma
It accounts for about one-third of all primary lung malignancy. Most of these tumors arise in a central location, the remainder in smaller bronchi.
Rare variants:
- papillary
- clear cell
- small cell
- basaloid
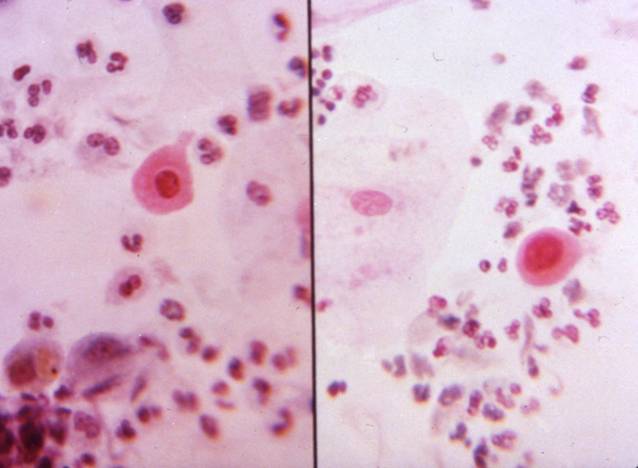
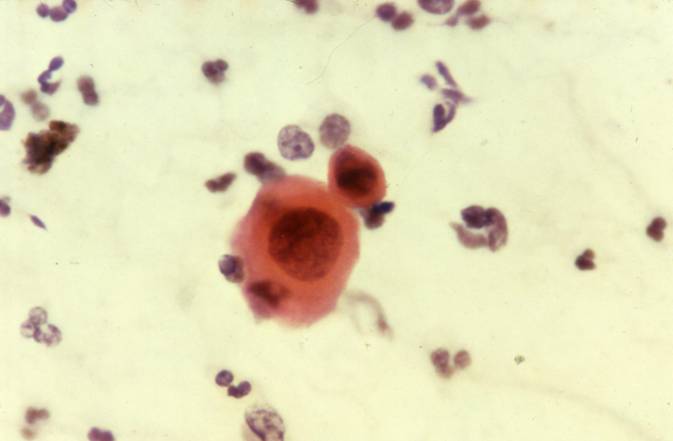
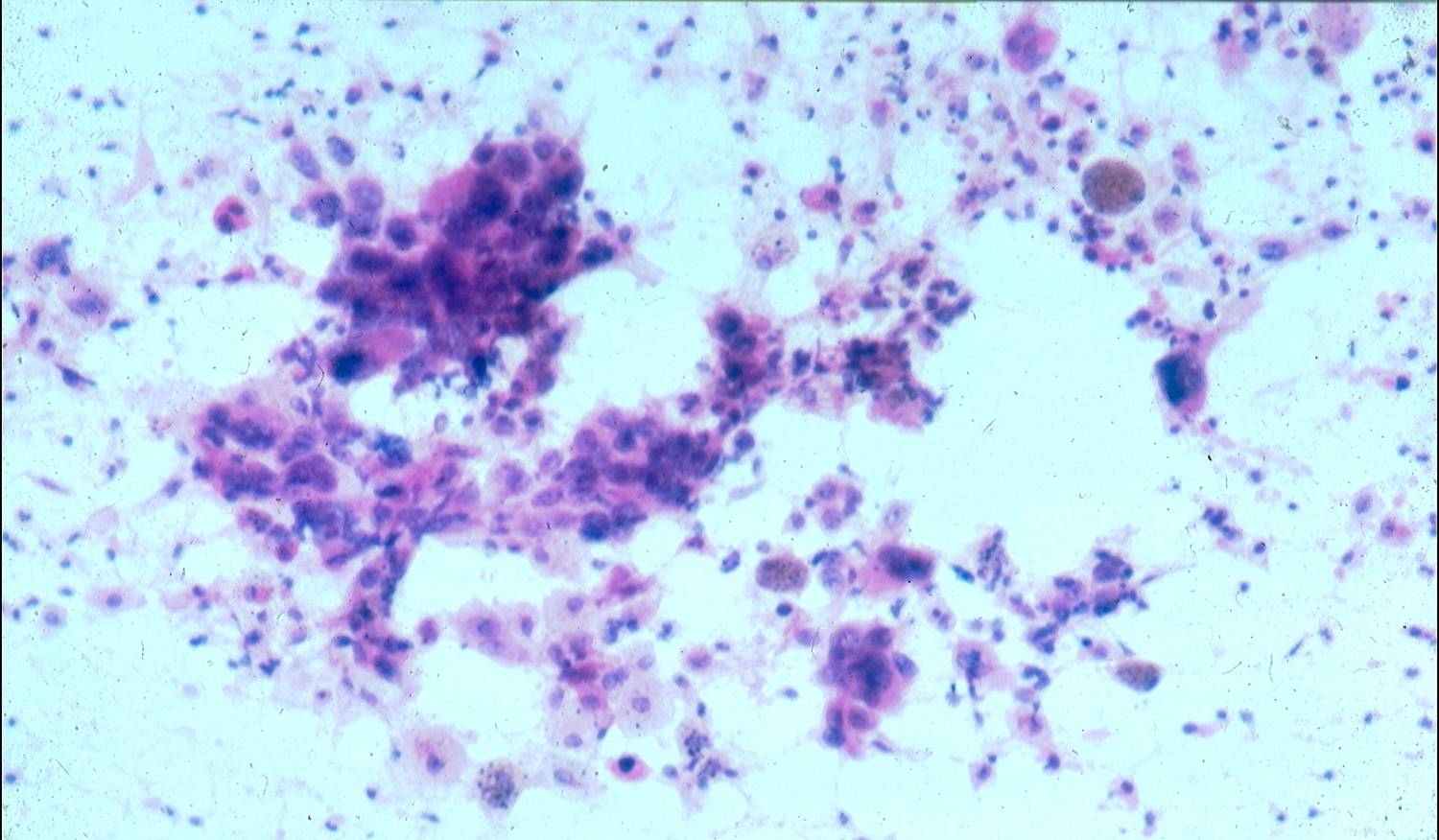
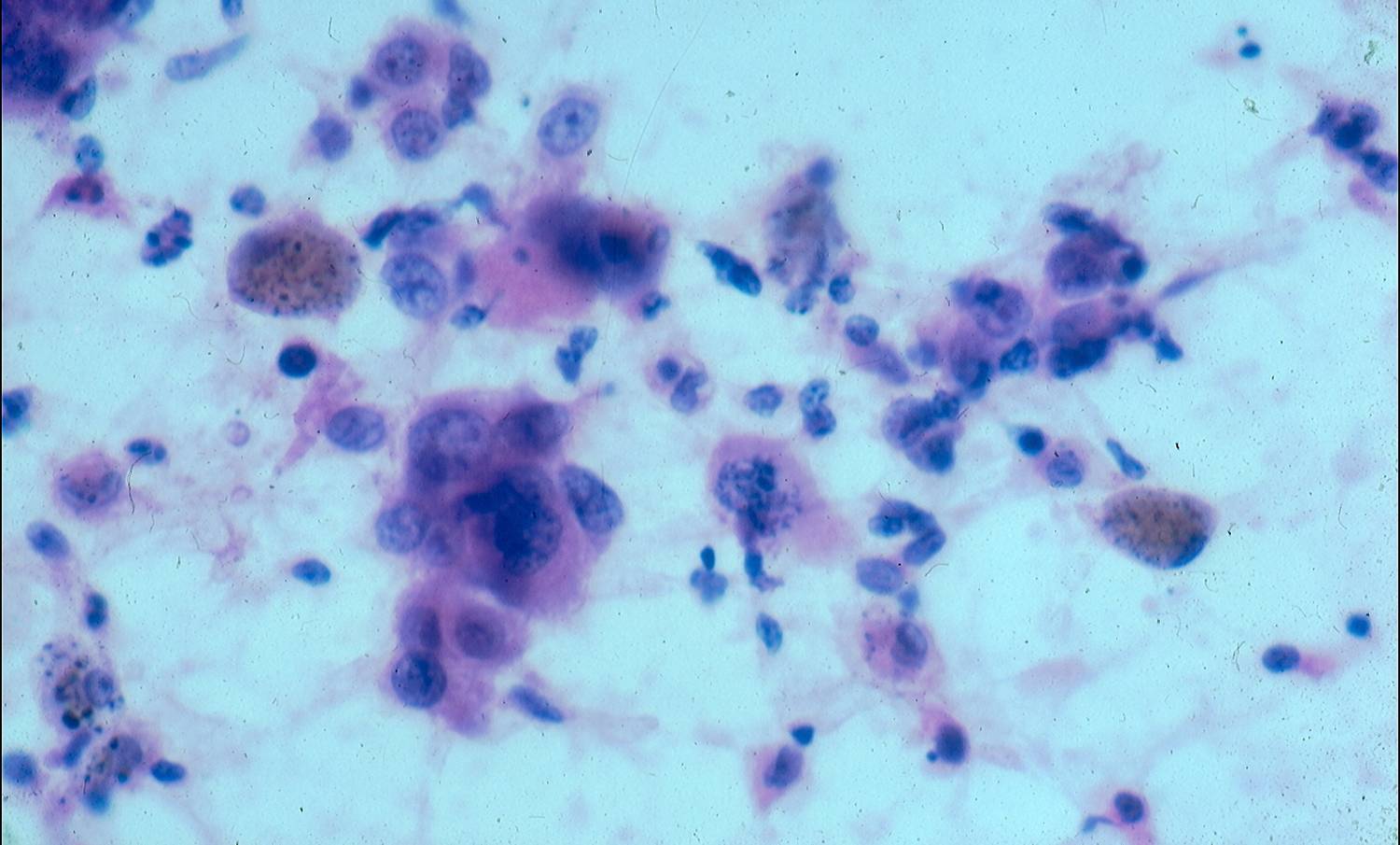
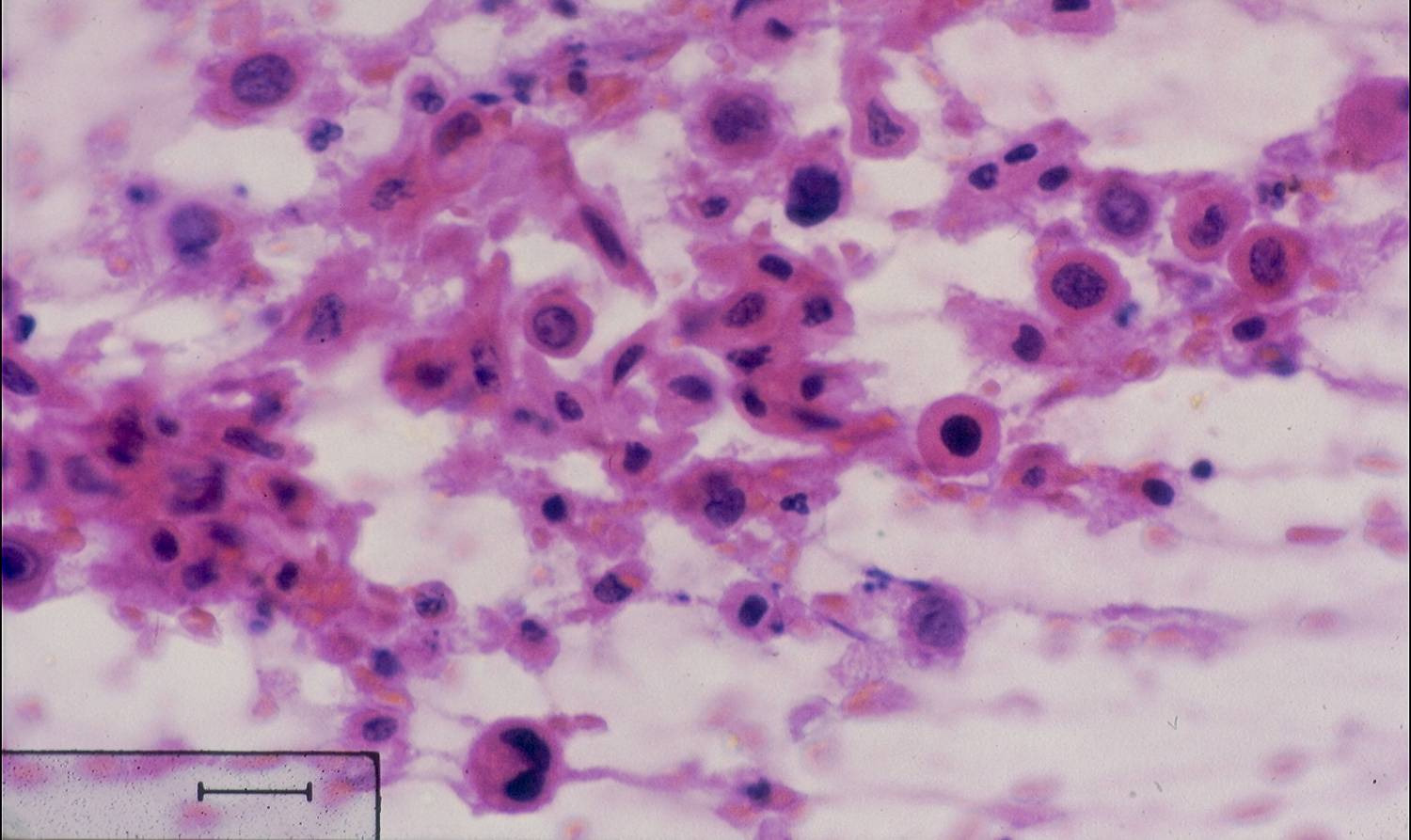
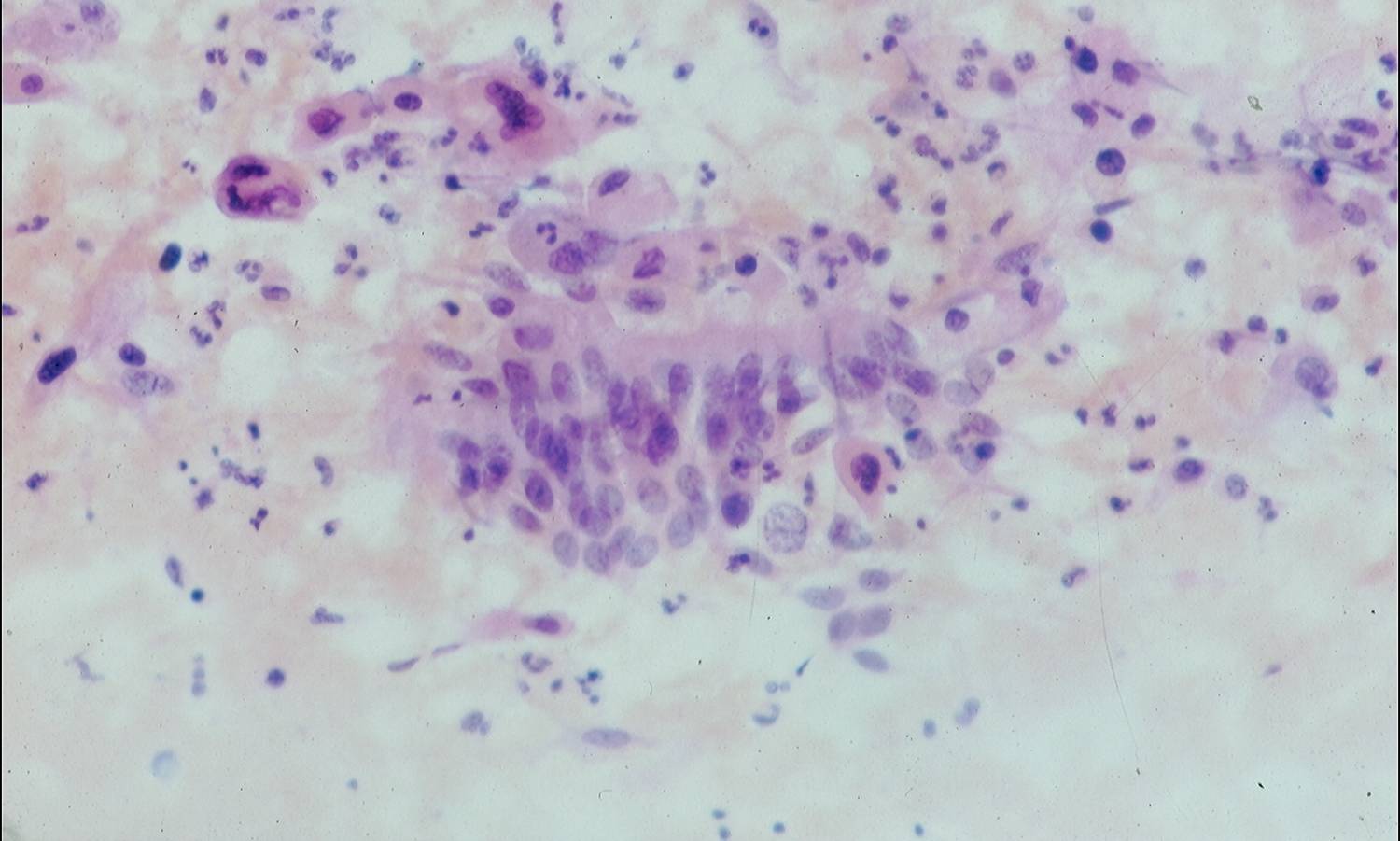
Cytologic diagnostic features (well-differentiated tumors)
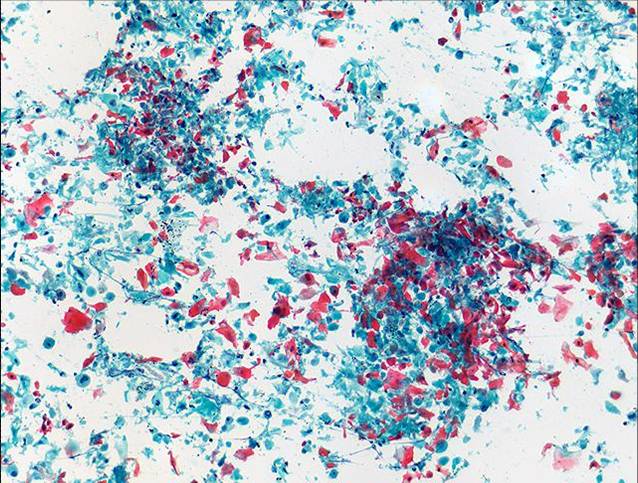
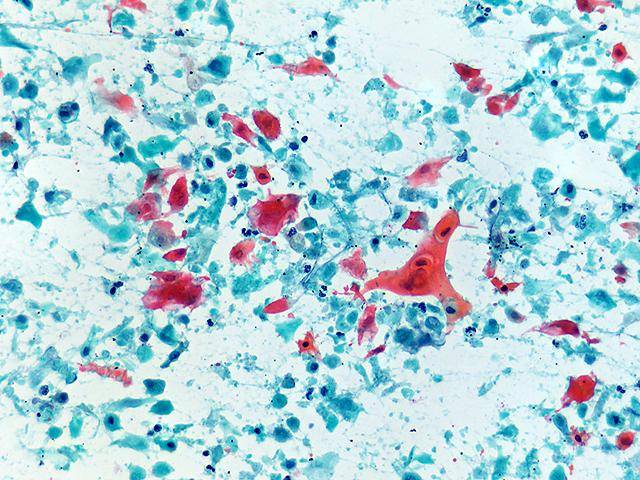
- Abundant dyshesive cells, that may be polygonal, rounded or elongated
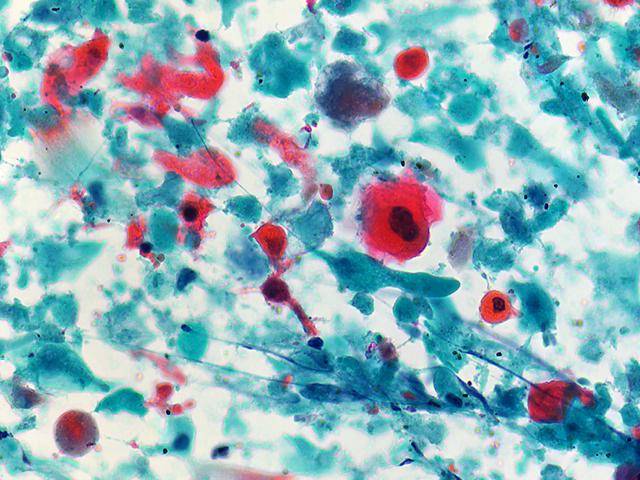
- Dense cytoplasmic orangeophilia (Papanicolaou stains)
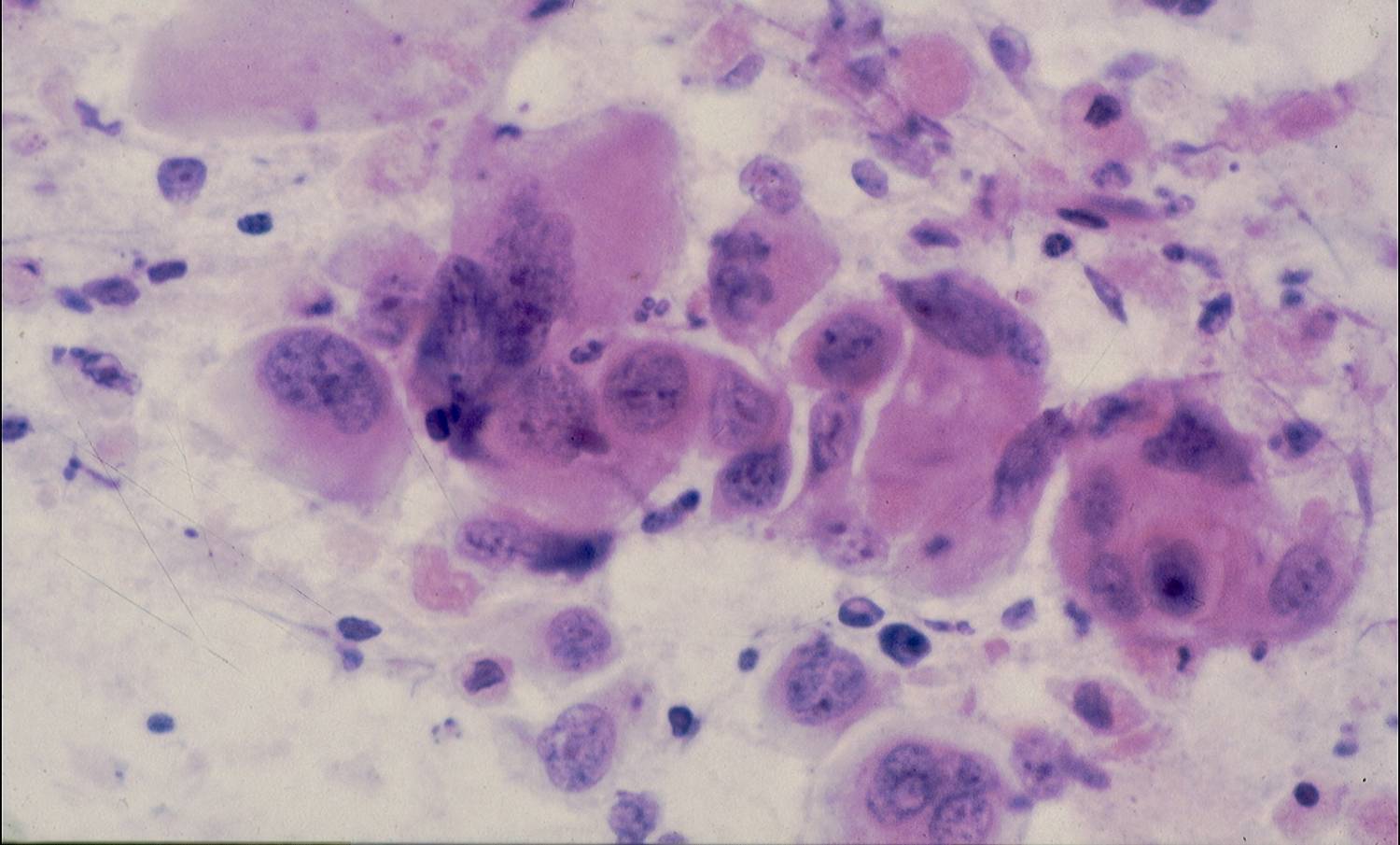
- Pleomorphic, hyperchromatic and often pyknotic nuclei
- Obscured nucleoli and chromatin detail
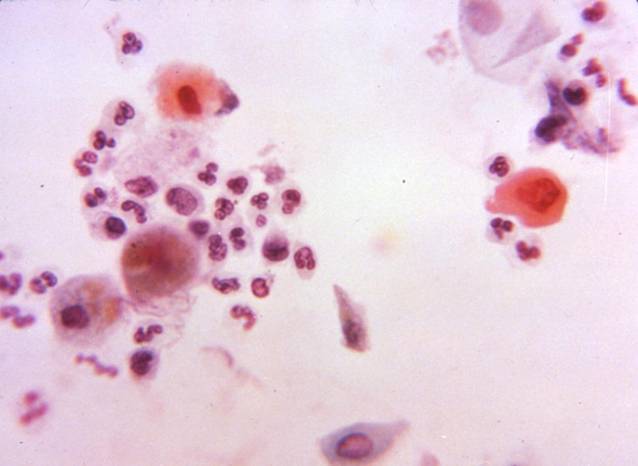
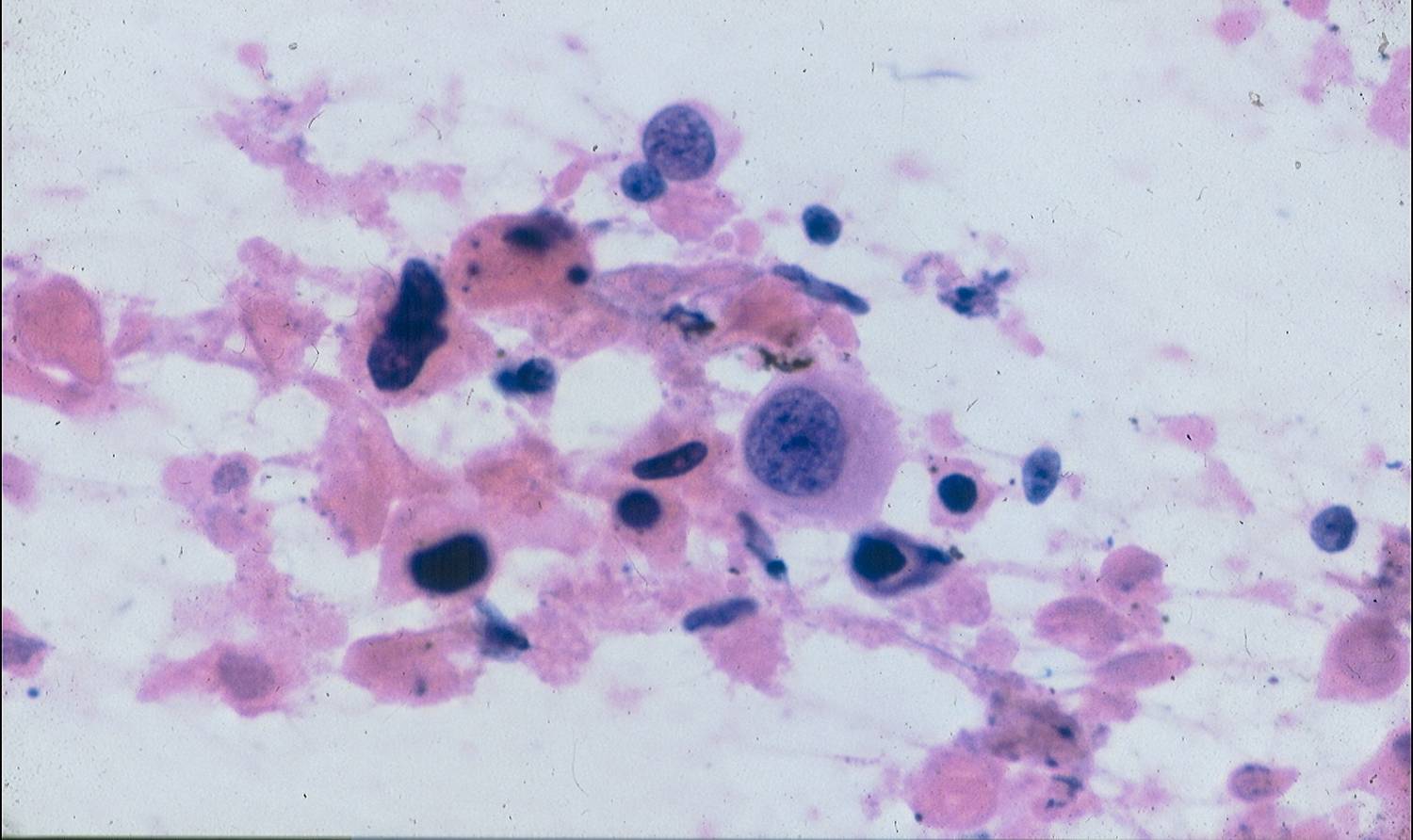
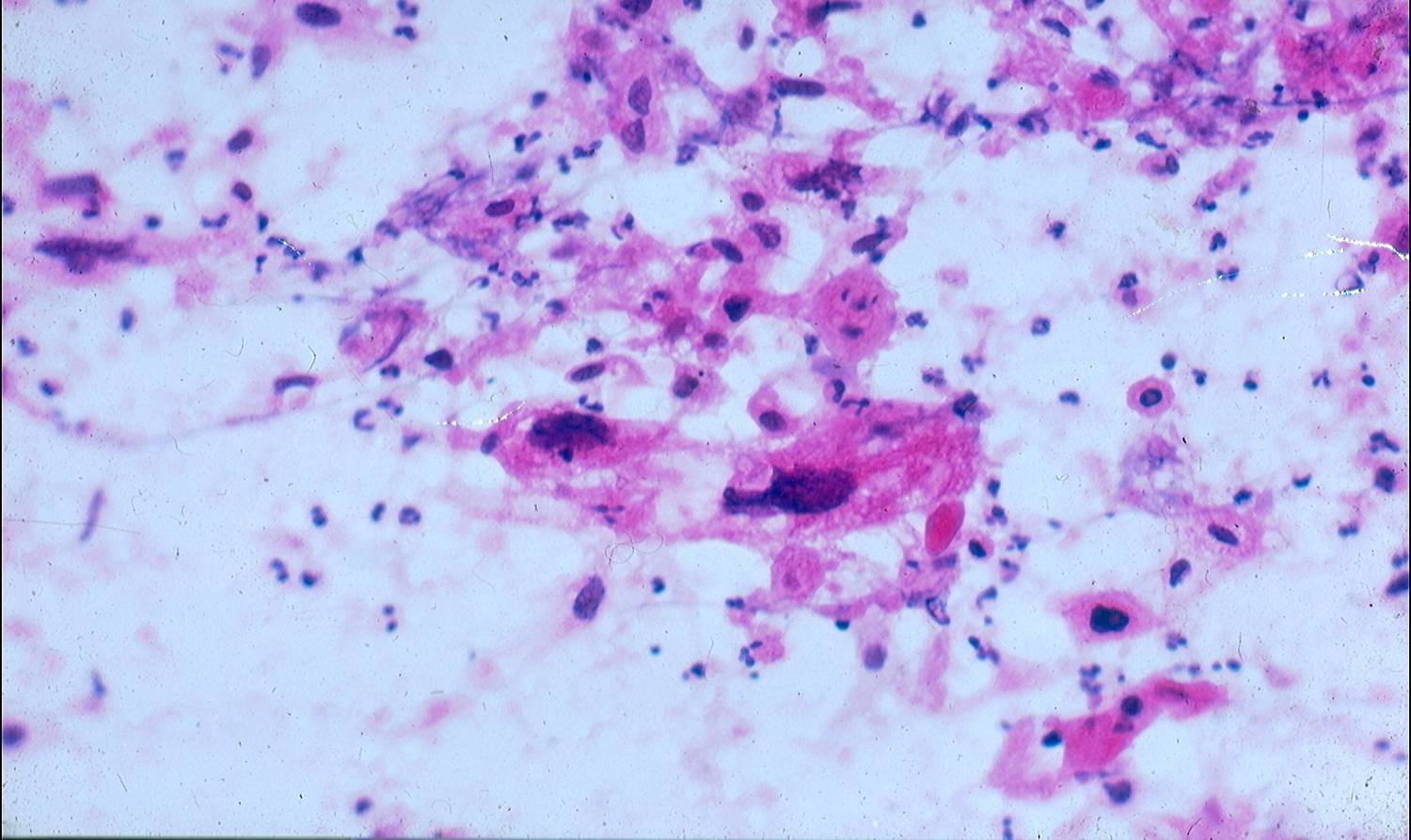
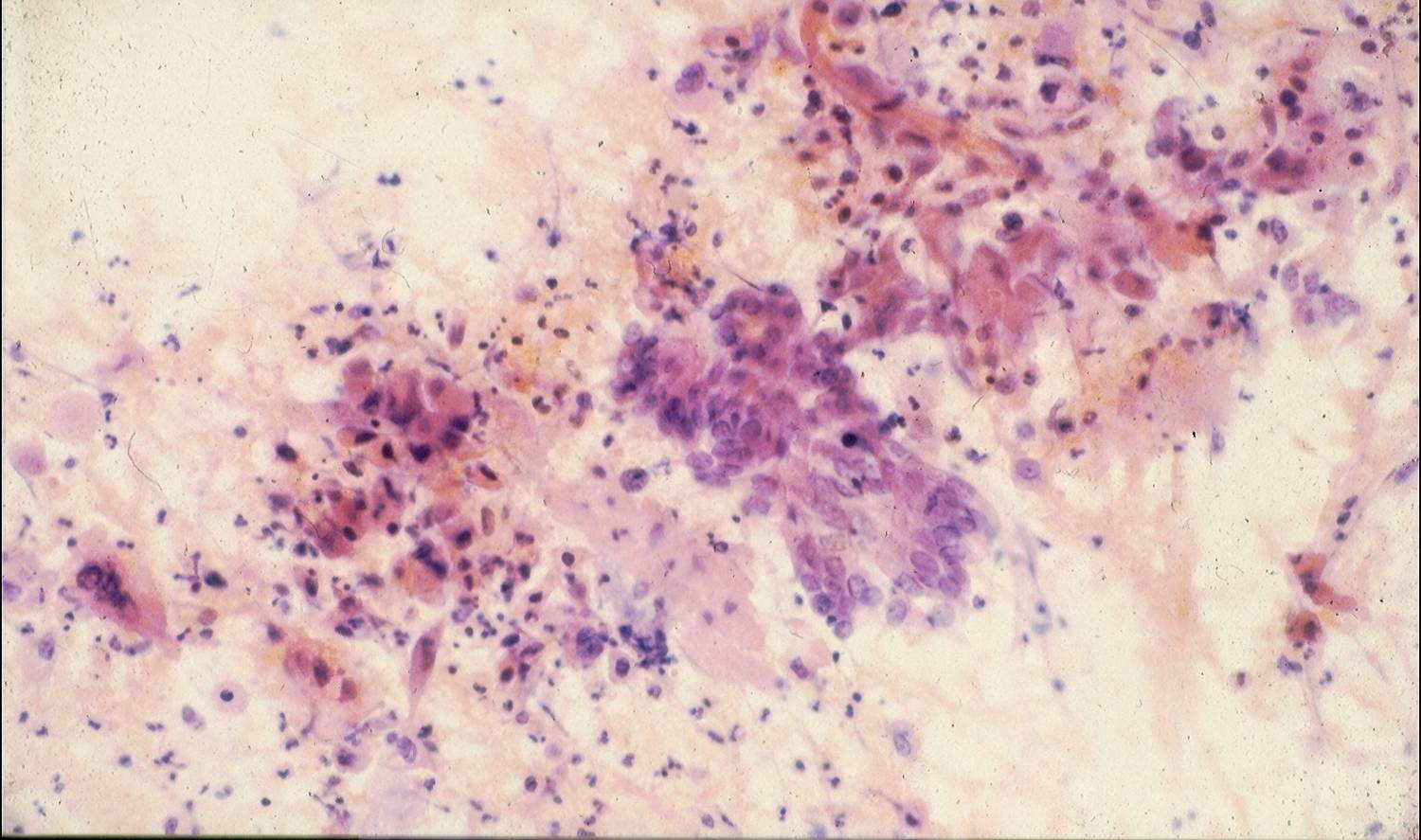
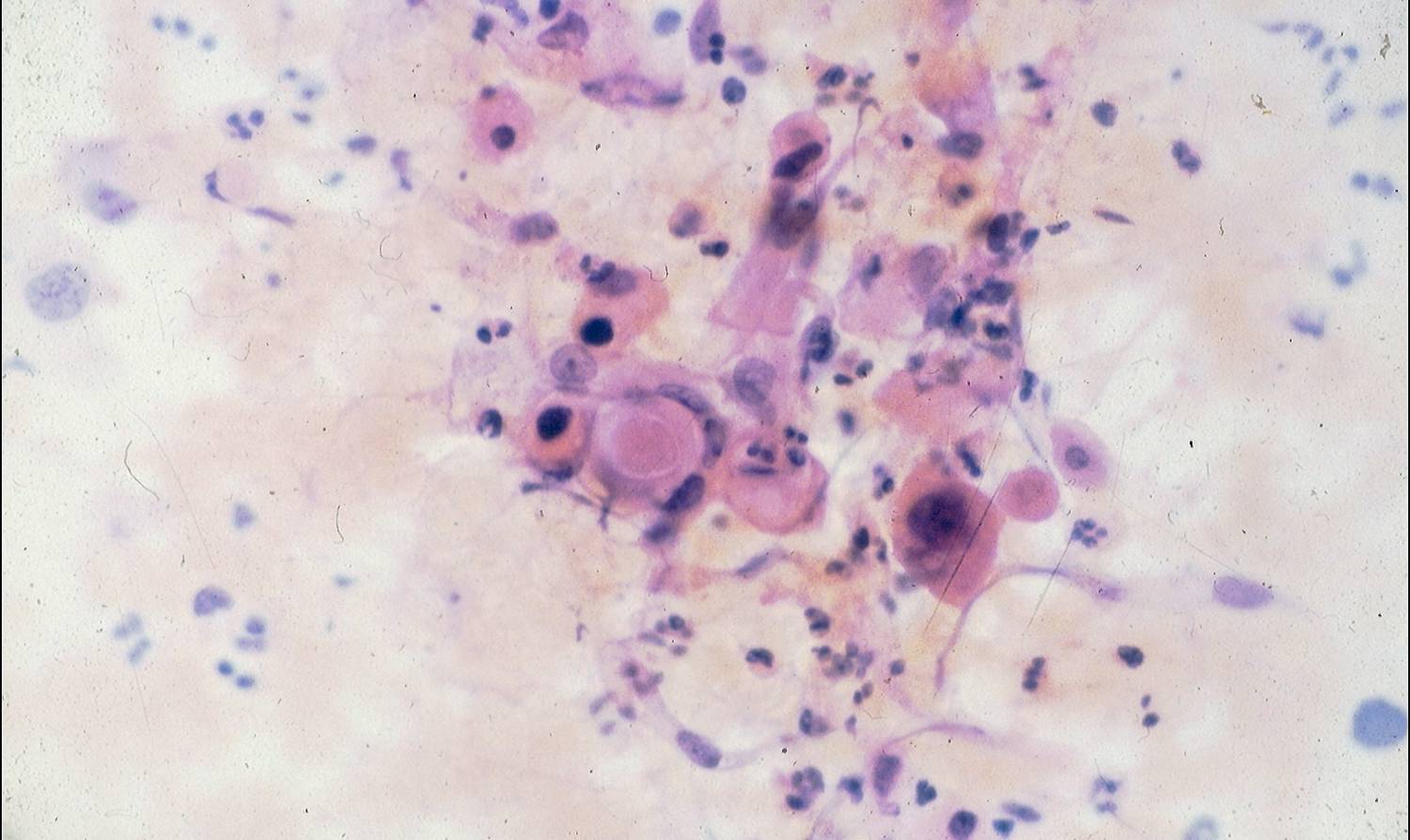
- Tadpole or fiber-like cells
- Frequent anucleate cells
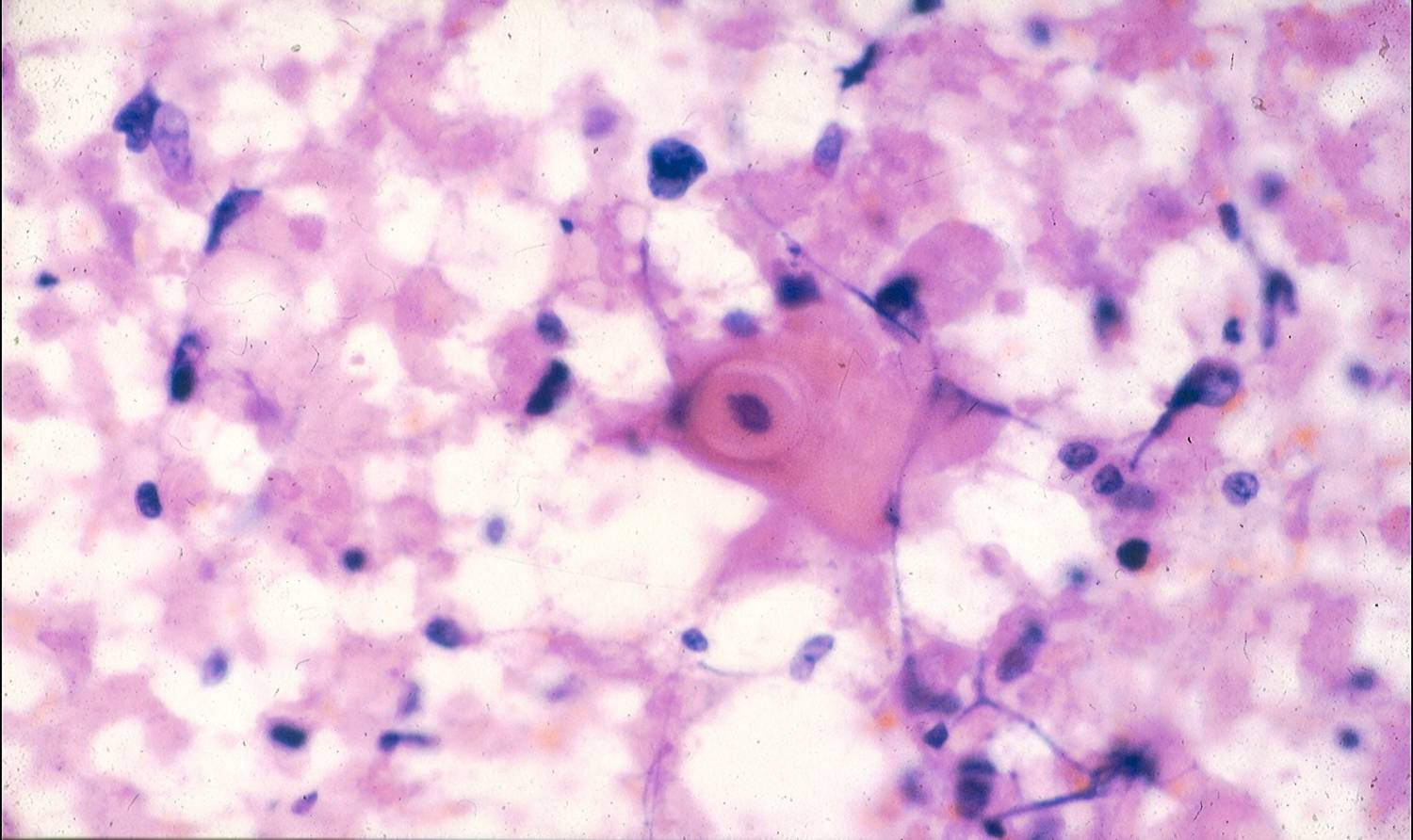
- Twisted keratin strands (Herxheimer spirals)
Tadpole or fiber-like cells are bizarre, elongated, spindle-shaped cells which can often be seen. An abundant granular debris, necrosis and inflammation are common.
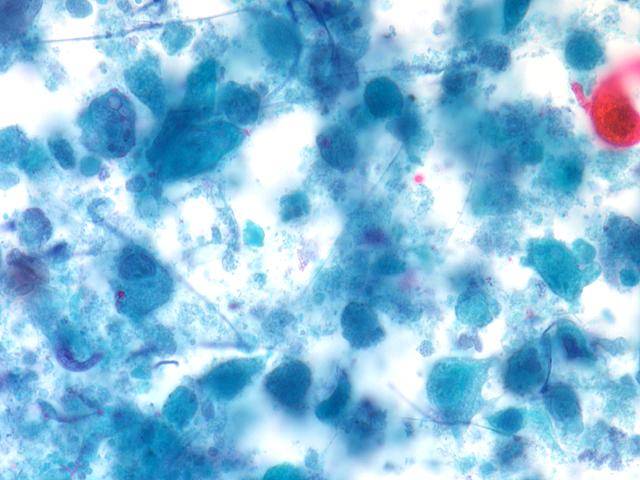
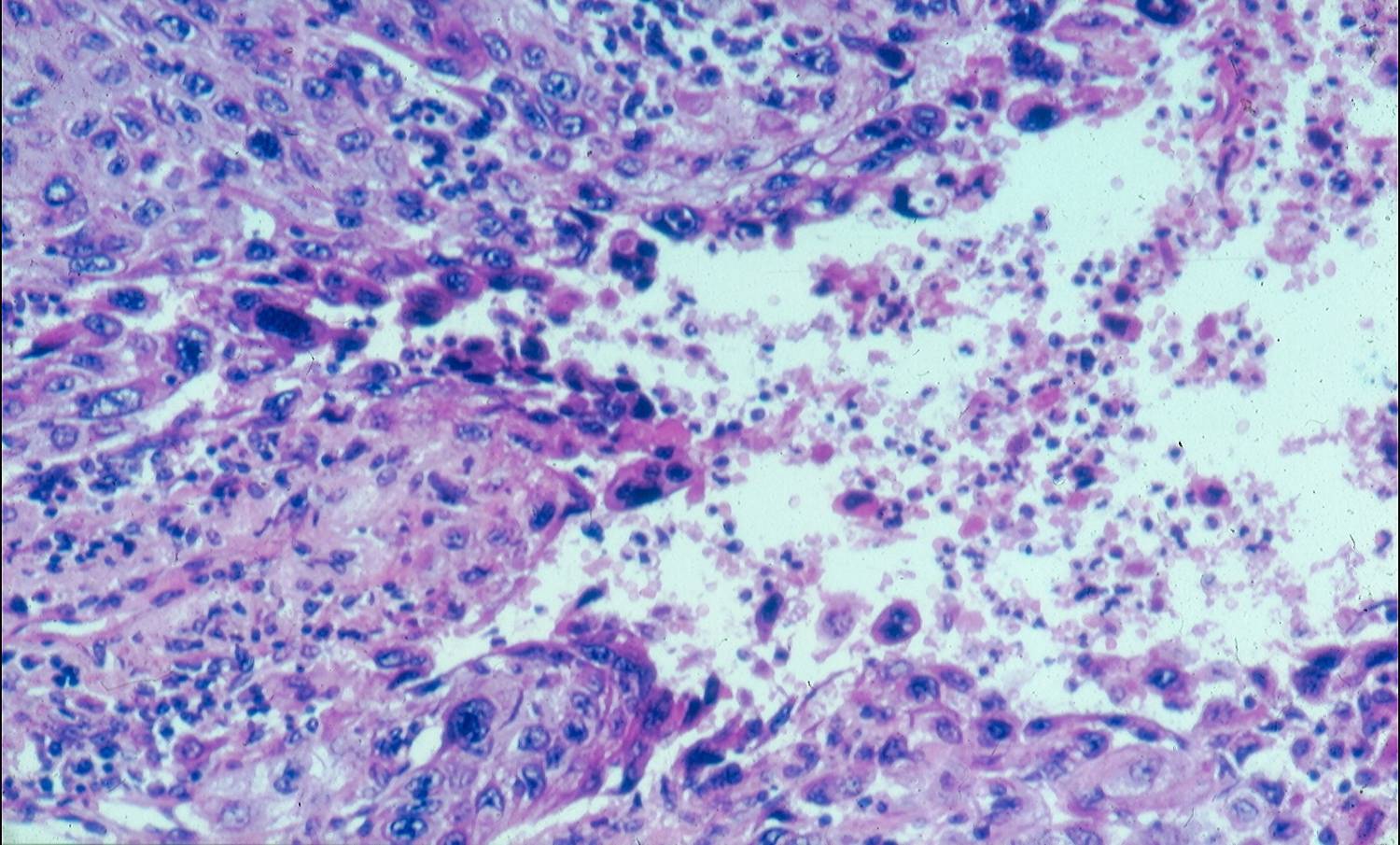
The cells of moderately or poorly differentiated tumors show larger nuclei with coarse and granular chromatin texture and cyanophilic cytoplasm (with Papanicolaou stains); they are often arranged in thick groups. Keratinization is rare or absent. In poorly-differentiated tumors a definitive diagnosis of squamous cell carcinoma can be sometimes hard to be made; a diagnosis of non-small cell carcinoma should be made in these cases.
False-positive diagnosis may occur as a result of overinterpretation of reparative or metaplastic changes. False-negative diagnoses may occur when only necrotic and inflammatory material is obtained.
Differential diagnosis
- Repair
- Squamous metaplasia
- Degeneration
- Mesothelial cells
- Radiation/chemoterapy effect
- Upper airway cancer contamination
Immunocytochemistry
- Cytokeratin 7 –
- Cytokeratin 5 +
- Cytokeratin 20 –
- Neuroendocrine markers –
- TTF-1 –
FNA FNA well differ histology
FNA well differ FNA well differ