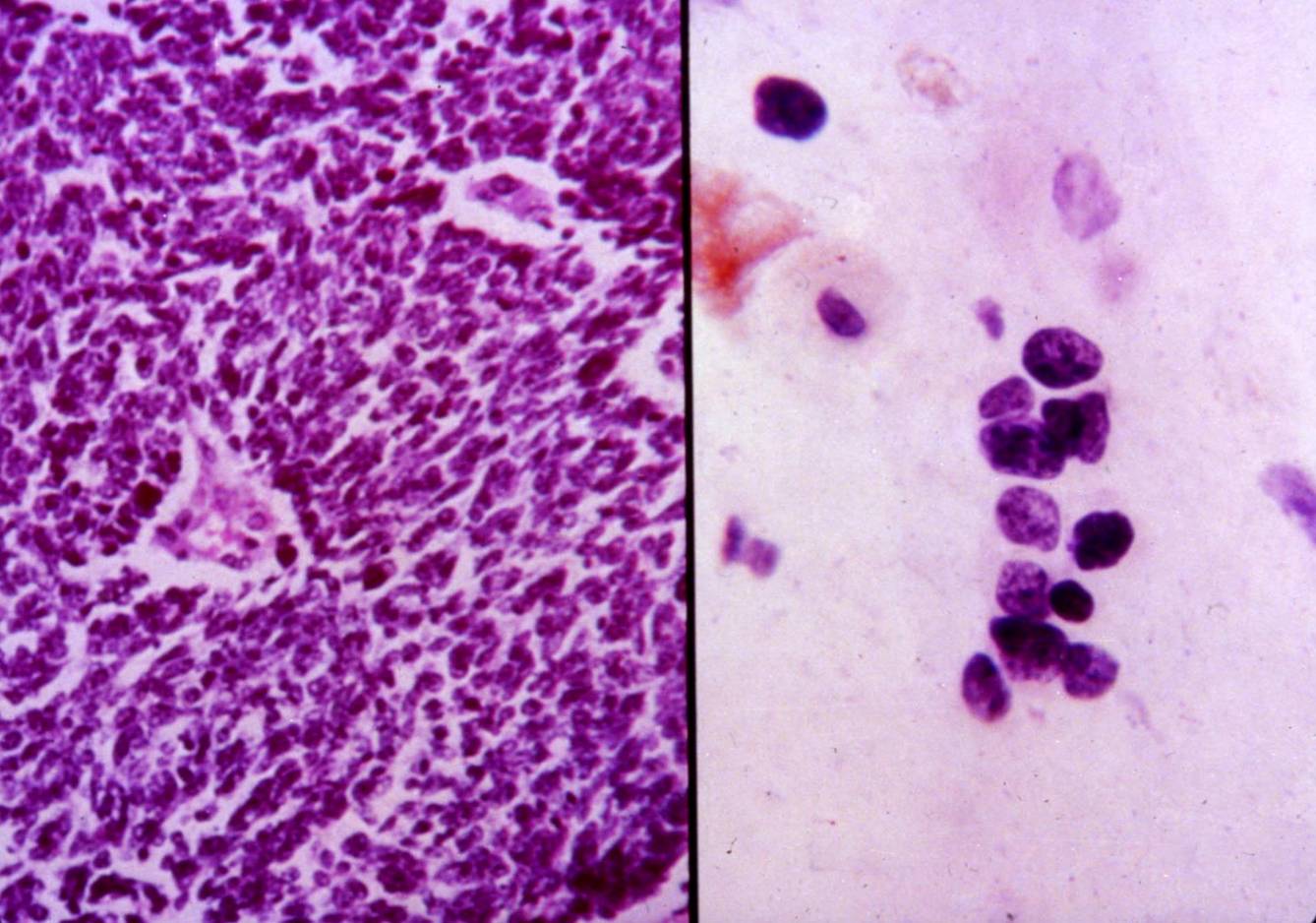
Small cell carcinoma
It accounts for about 20-25% of primary lung carcinomas; most of the patients are smokers. This tumor is often widely metastasizing and the prognosis is poor.
Small cell carcinoma is a neuroendocrine neoplasm; ultrastructurally, the cells contain cytoplasmic dense-core granules which stain positive with neuroendocrine markers (such as chromogranin).Small cell carcinoma is classically composed of small, round to fusiform cells with scant cytoplasm. Necrosis, a high mitotic rate and nuclear encrustation of vascular walls are characteristic features. Cells of intermediate variant are larger, with more cytoplasm and vesicular nuclei.
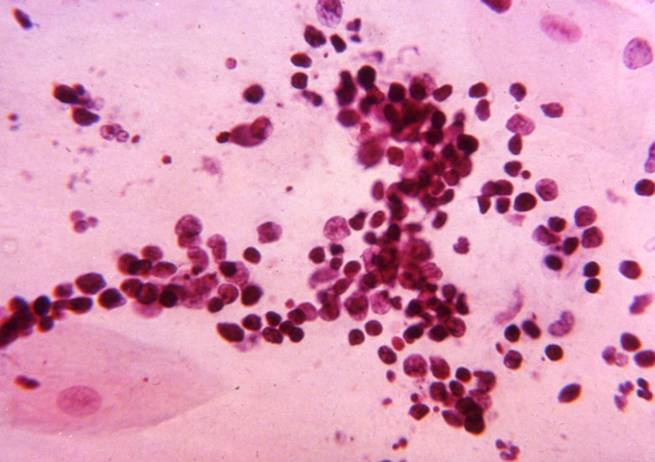
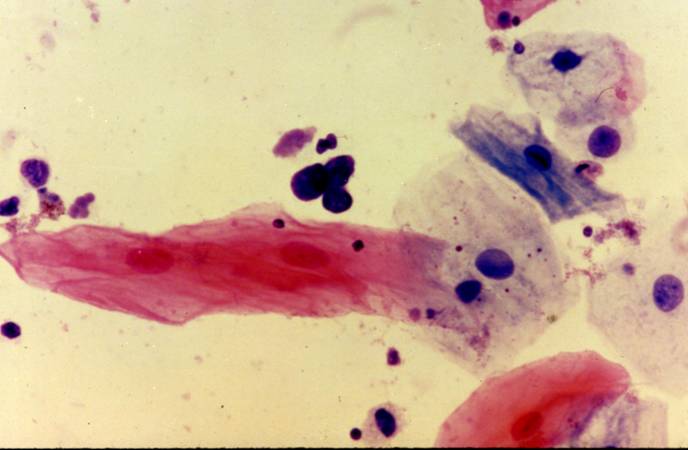
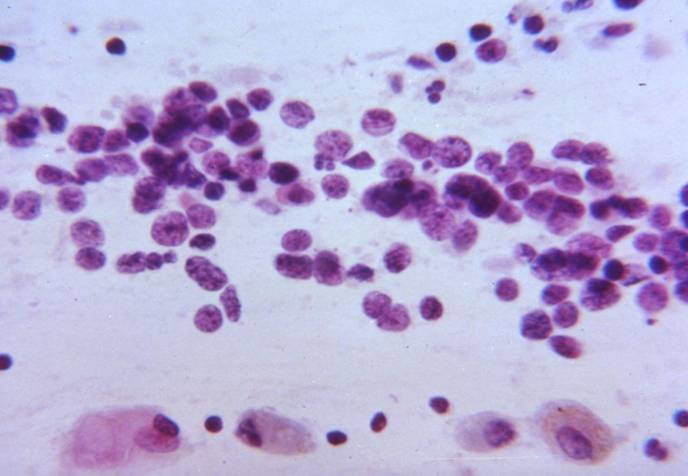
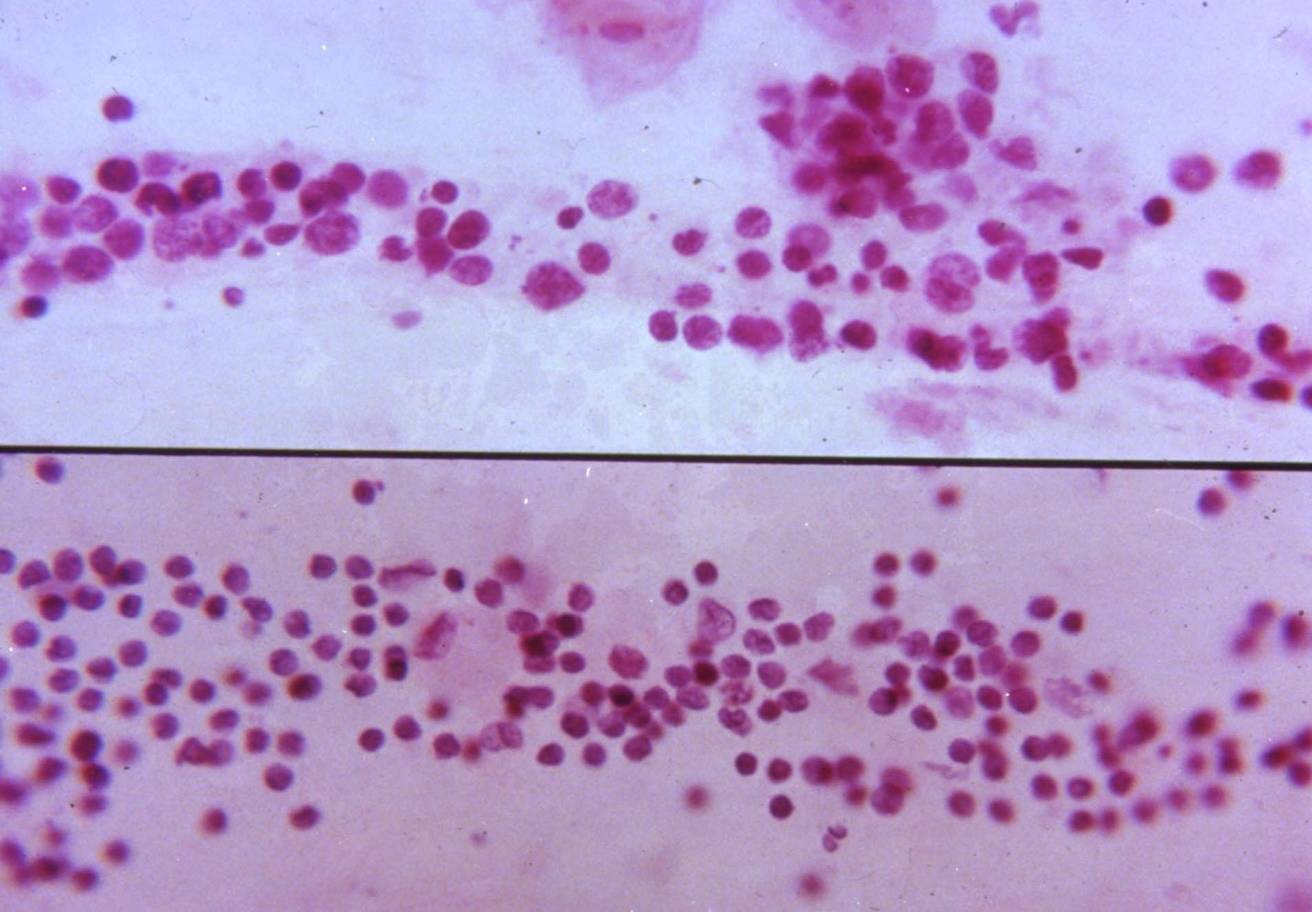
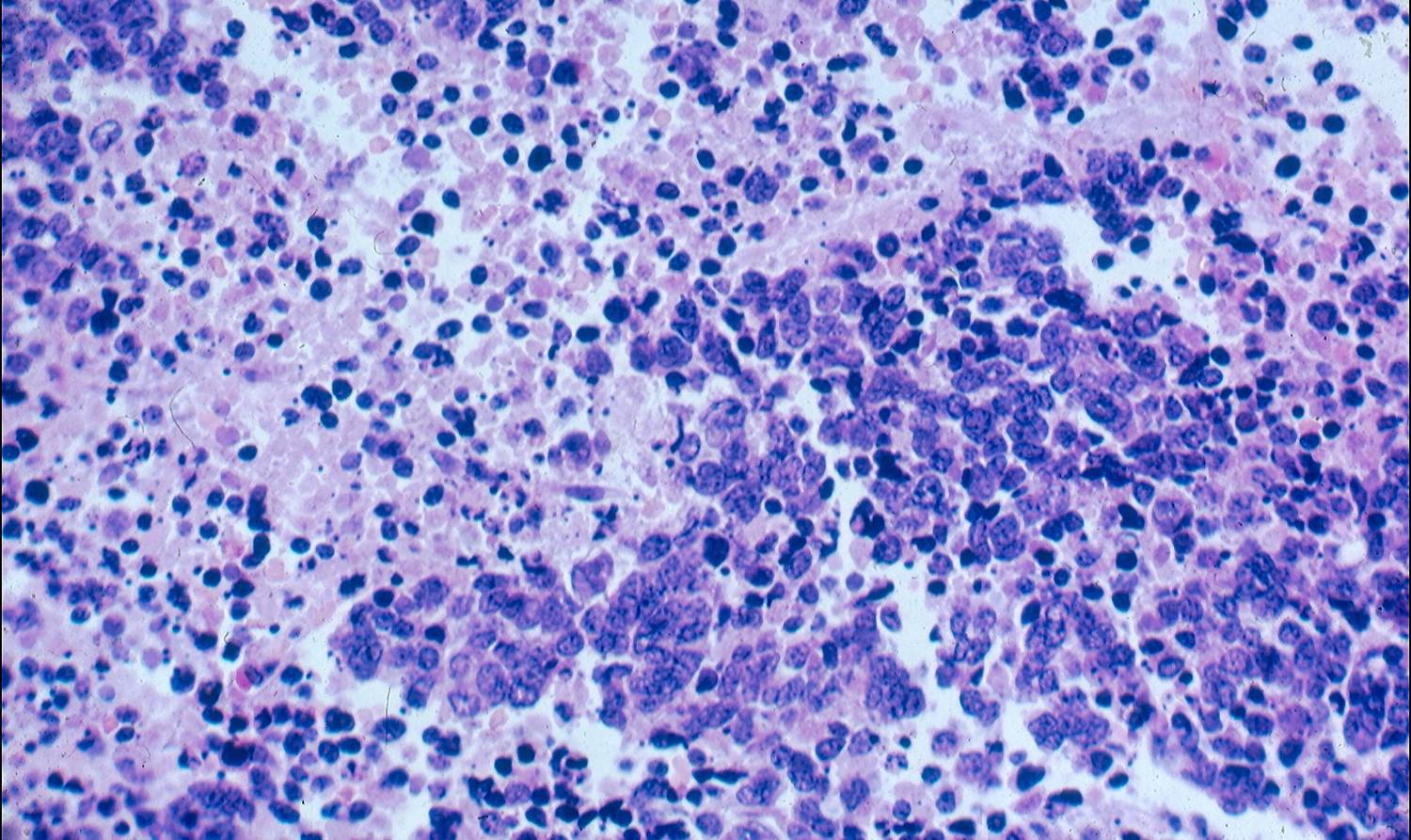
Cytologic diagnostic features (sputum and bronchial washing)
- Enlongated grouping of small dissociating tumour cells (twice the size of lymphocytes; occasionally larger)
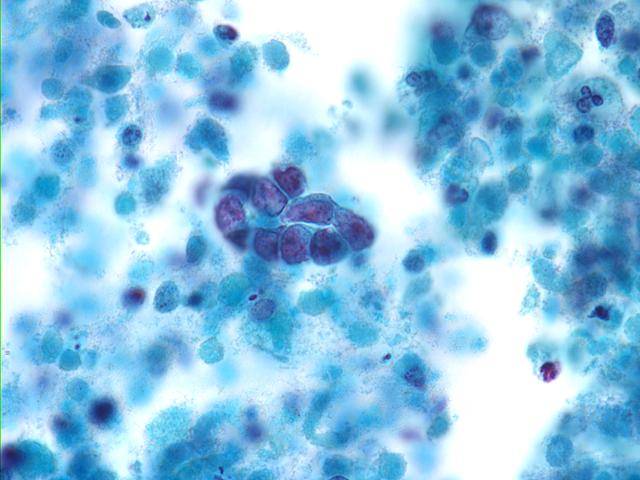
- Scanty cytoplasm, irregular carrot-shaped, hyperchromatic nuclei, showing molding
- Coarse chromatin, incospicuous nucleoli
- Mitosis
- Degenerative changes
- Local tumour diathesis
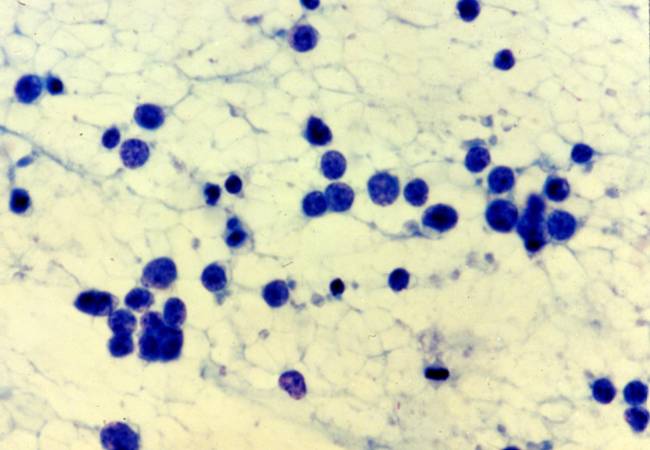
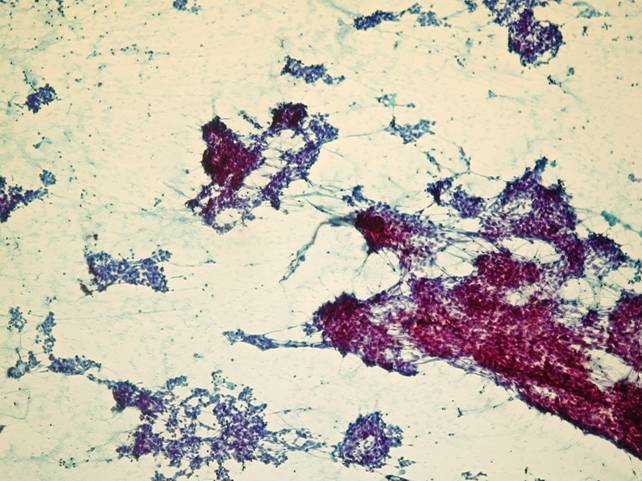
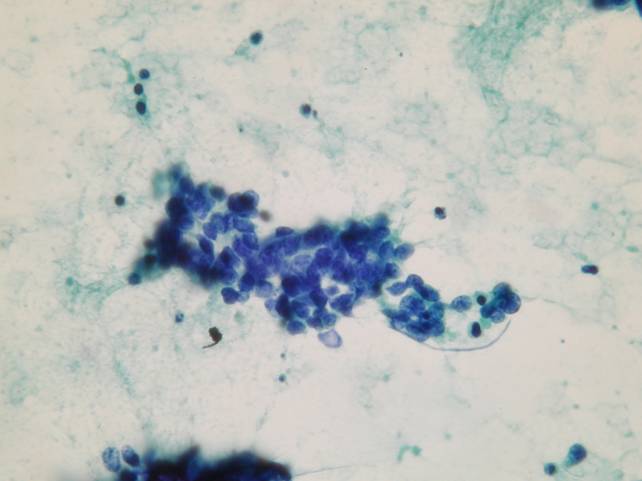
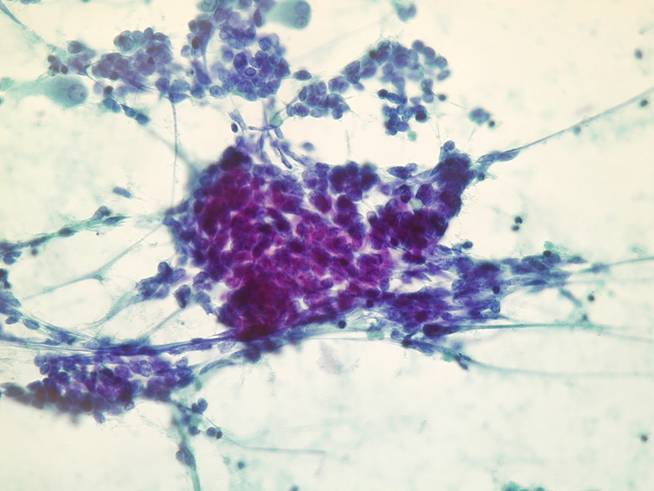
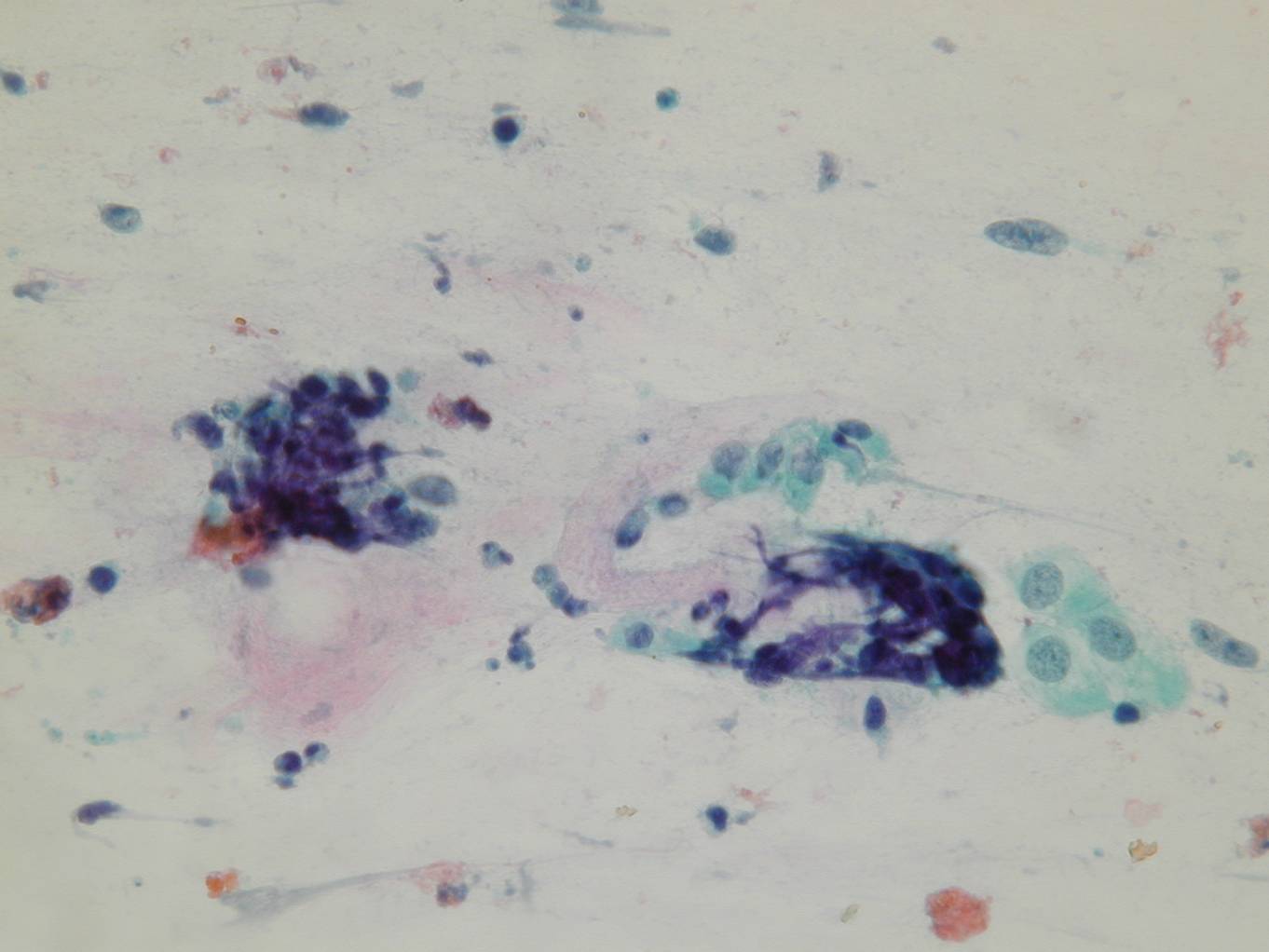
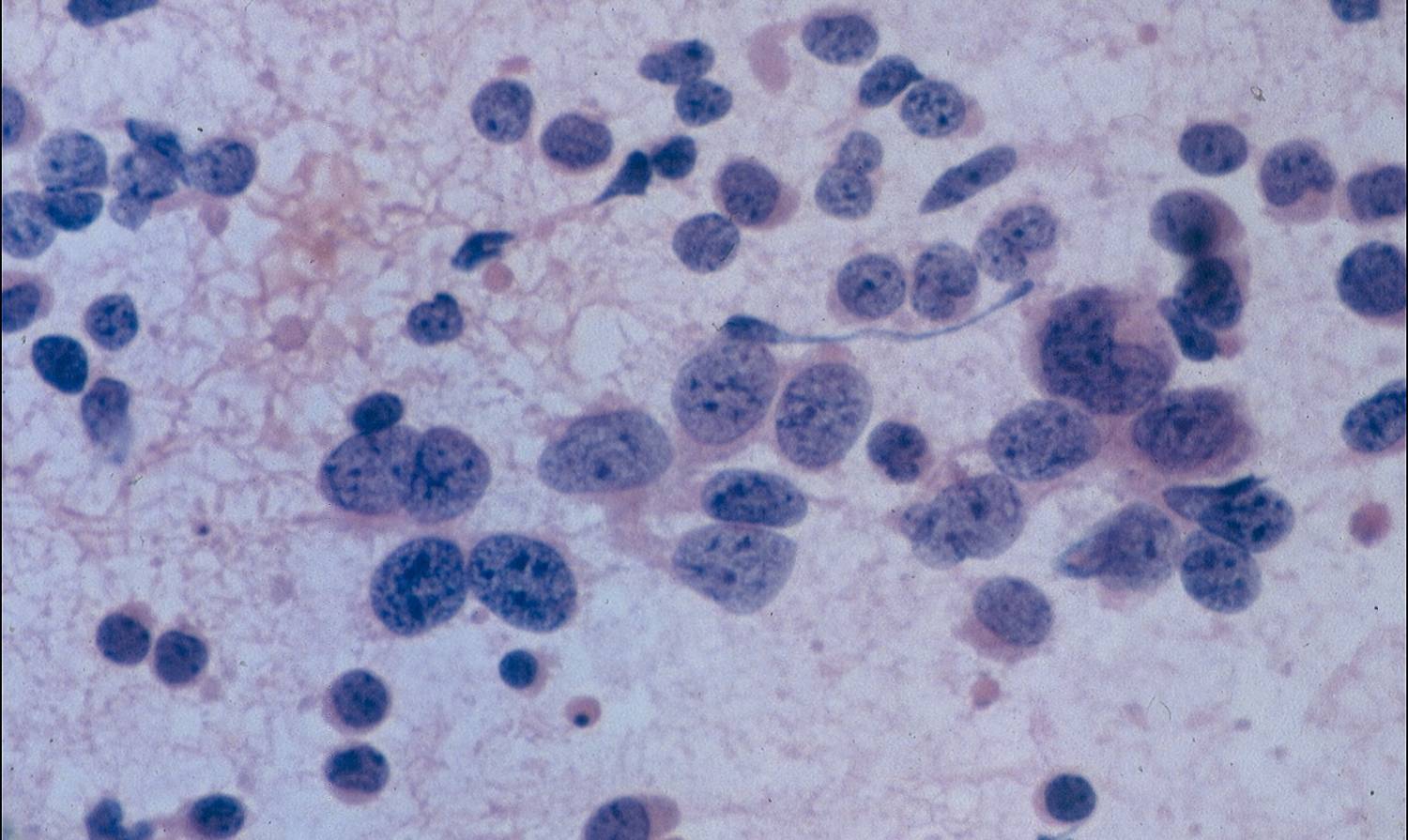
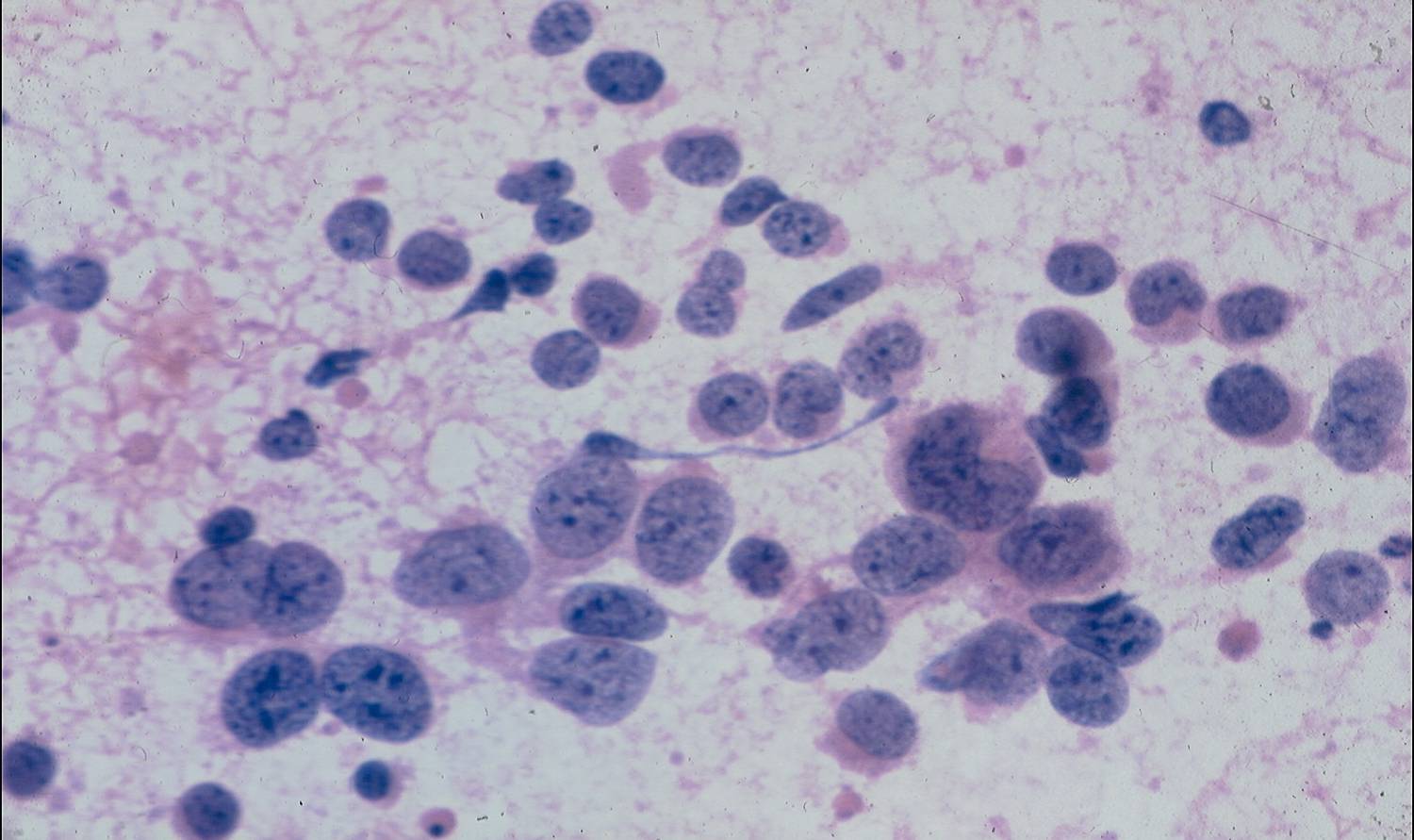
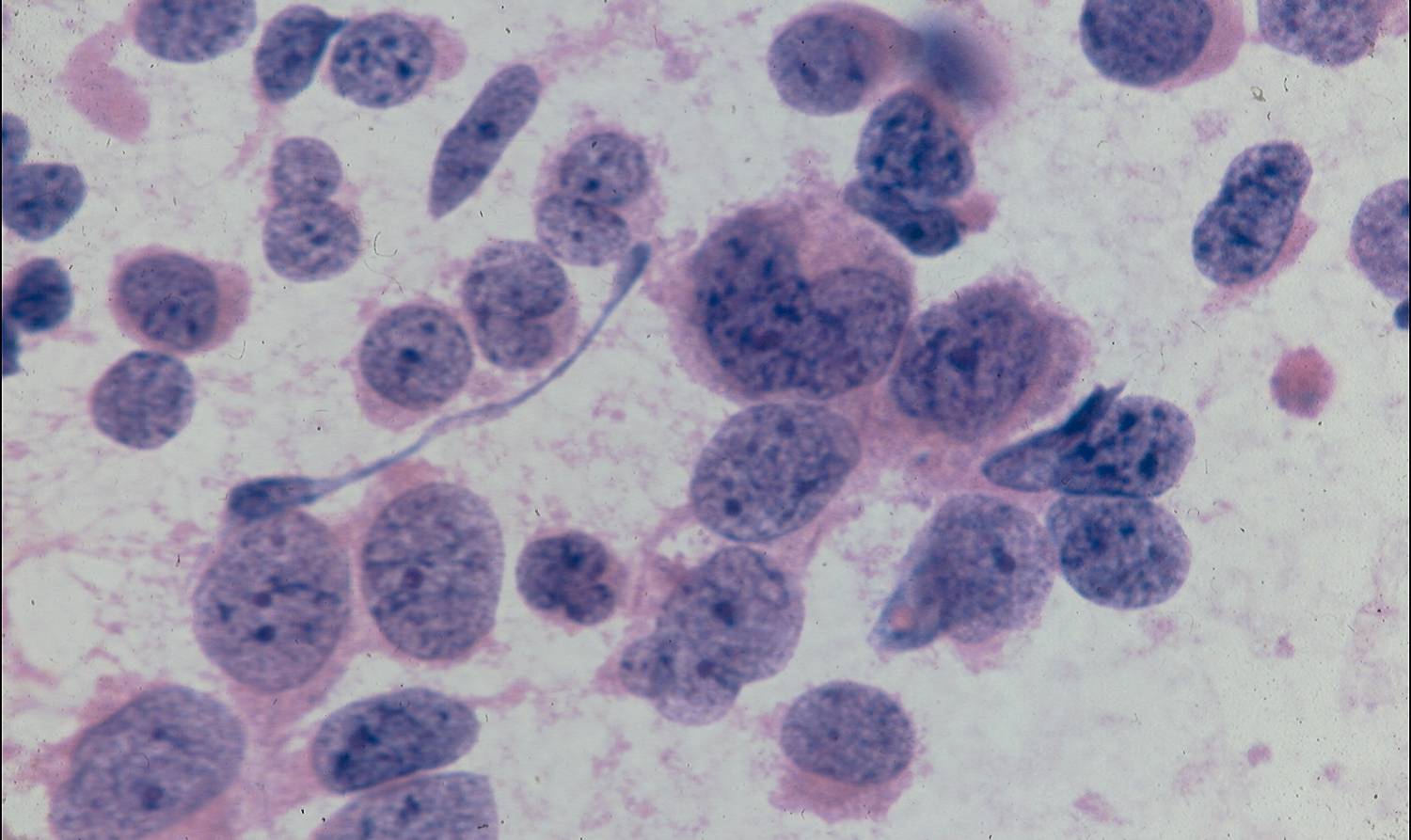
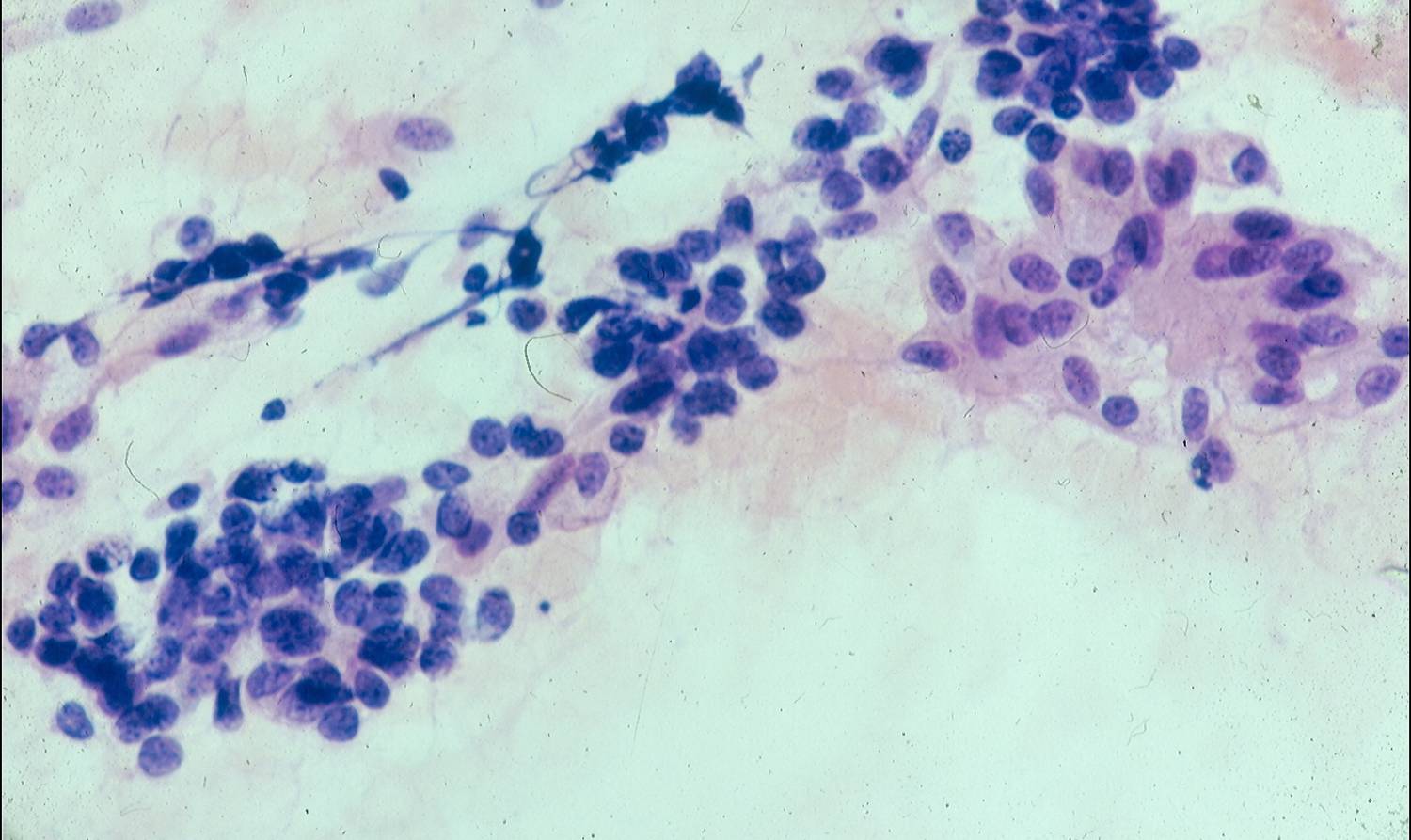
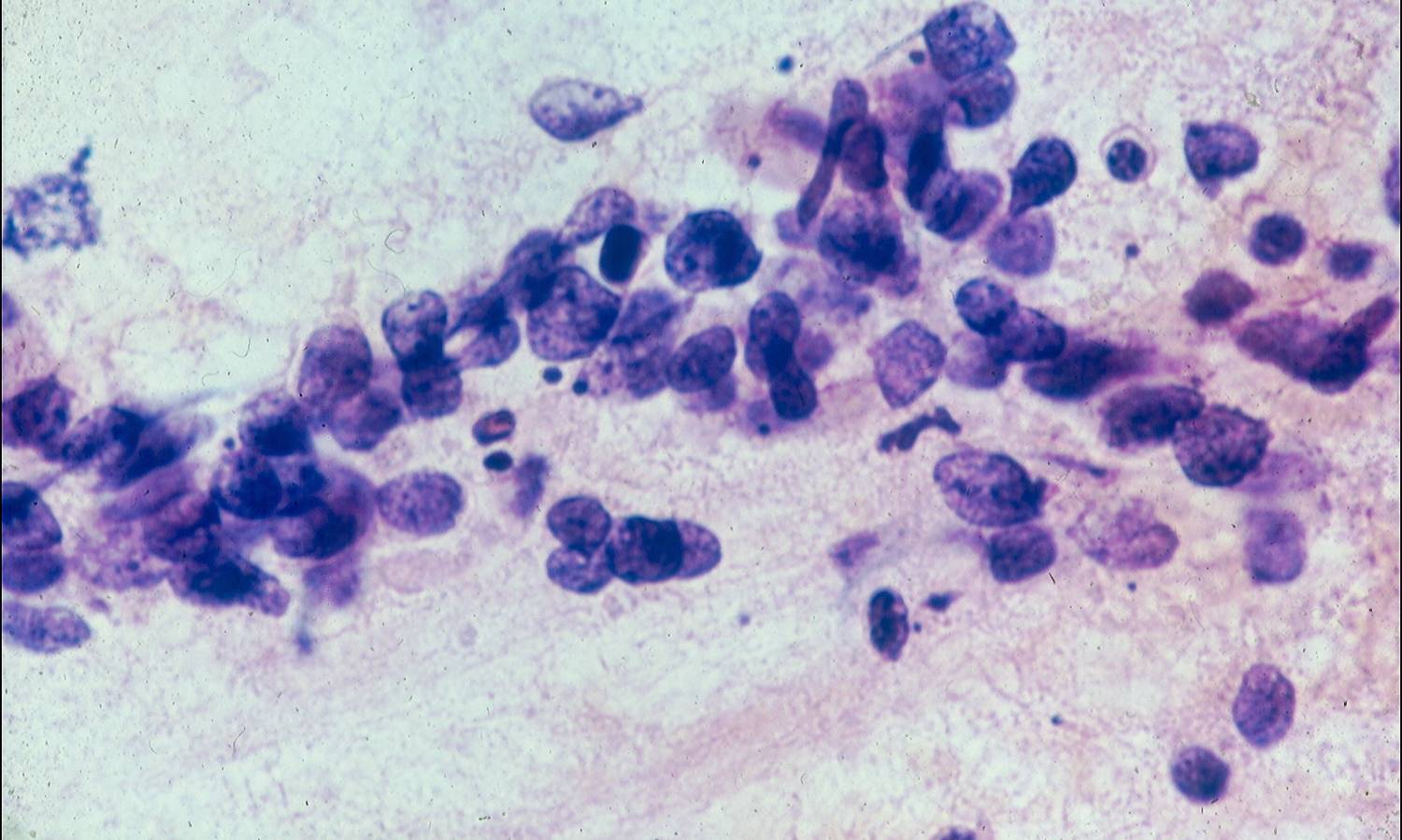
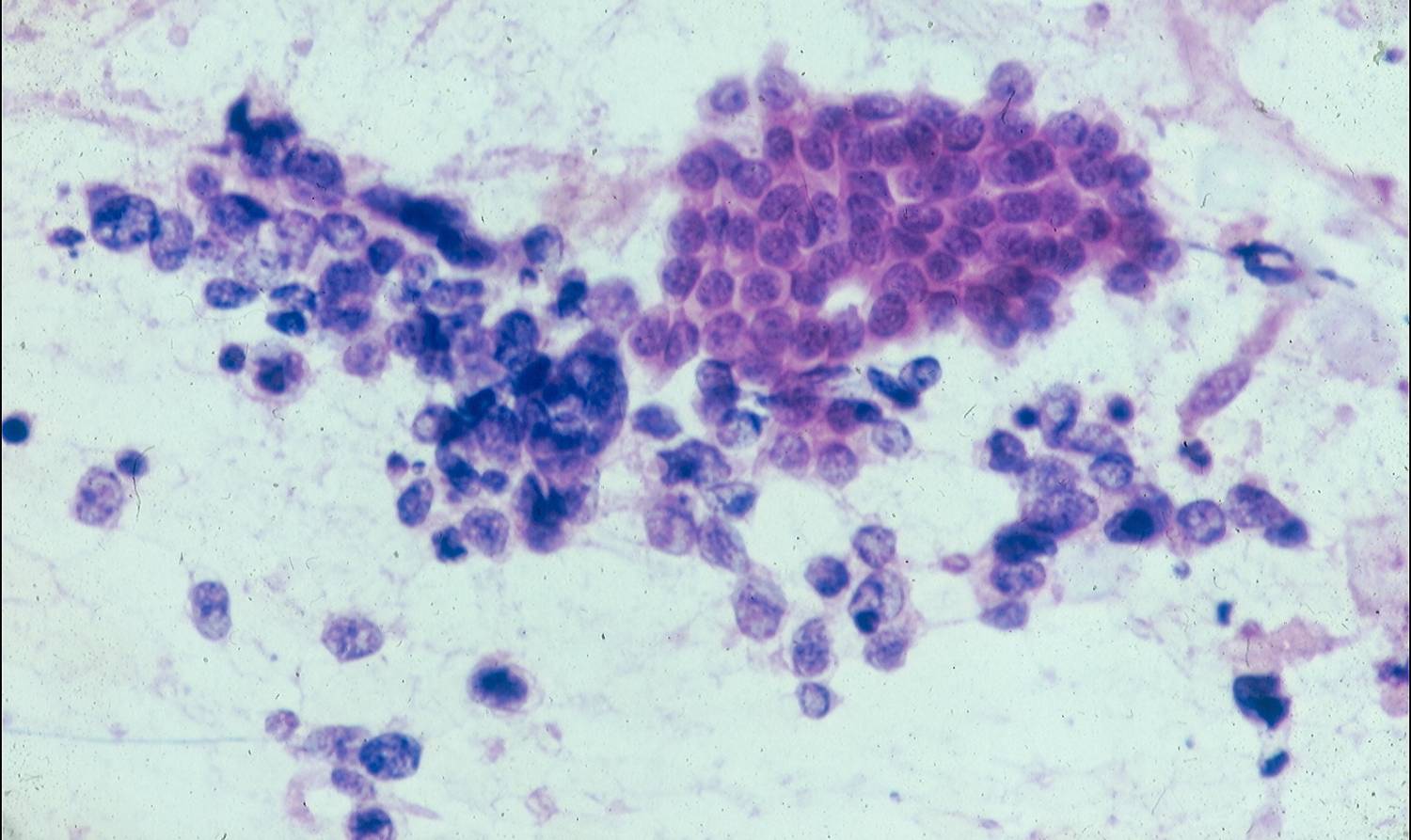
Cytologic diagnostic features (FNA and bronchial brushing)
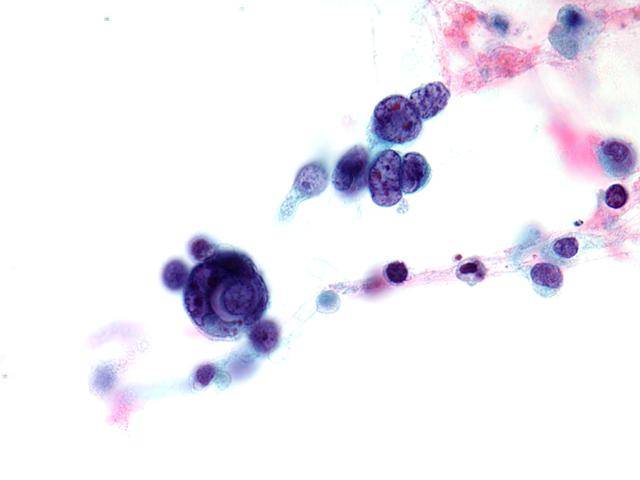
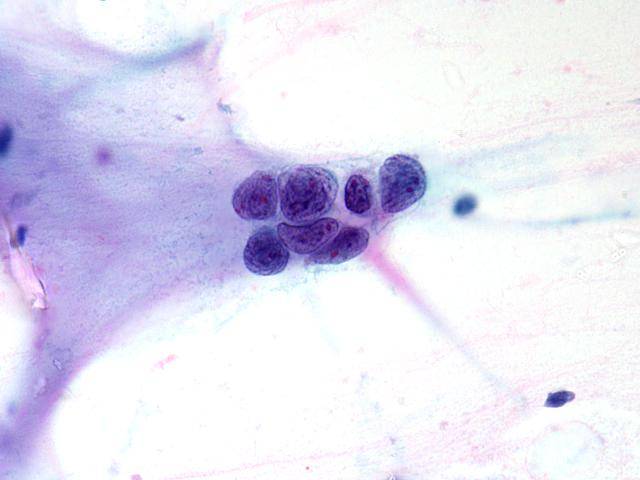
- Better preserved larger cells than in sputum (oval or spindly)
- Nuclear molding and clustering
- Large coarsely granular or pyknotic nuclei
- Open chromatin pattern
- Artefactually crushed cells and nuclei
Differential diagnosis
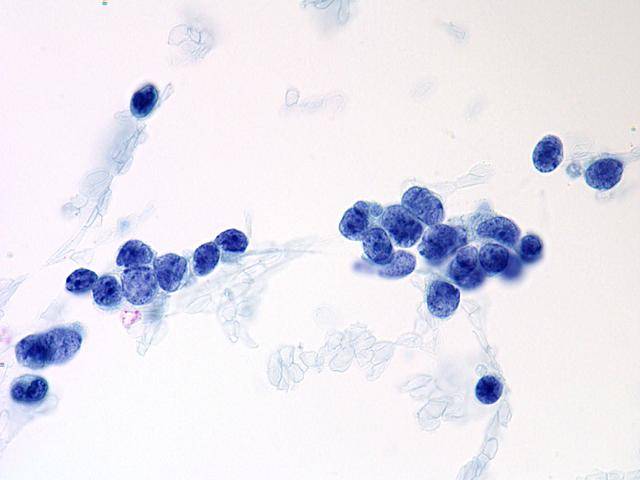
- Reserve cell hyperplasia
- Lymphocytes
- Pulmonary blastoma
- Carcinoid
- Non-small cell carcinoma
- Ewing`s sarcoma
- Neuroblastoma
The cells of reserve cell hyperplasia also show molding, but they are smaller and more cohesive than those of small cell carcinoma. Lymphoid cells, whether from an inflammatory process or a lymphoma, can be confused with a small cell carcinoma, but they usually do not form clusters and tend to be spaced, and when they are benign they are smaller than tumor cells. In carcinoid tumors nuclear molding, necrosis and mitotic activity are not observed, and the chromatin texture is more coarsely granular. The distinction between small cell carcinoma and an atypical carcinoid tumor is more difficult; usually, small cell carcinomas have less cytoplasm, more nuclear molding and more finely granular chromatin texture. Small cell carcinoma must be distinguished from poorly differentiated non-small cell carcinomas, such as squamous cell carcinoma and adenocarcinoma. The powdery chromatin texture, incospicuous nucleoli and prominent nuclear molding are helpful diagnostic features of small cell carcinoma.
Immunocytochemistry
- Neuroendocrine markers + (Chromogranin A, CD56, NSE, Synaptophysin)
- Cytokeratin 7 +
- Cytokeratin 5 –
- Cytokeratin 20 –
- TTF-1 +
sputum sputum brush
FNA FNA FNA
reserve cell hyperplasia
FNA FNA histology