| Physiopathology of the effusions |
| Specimen collection and preparation methods |
| Accuracy |
| Reporting terminology |
| Benign elements |
| Non-neoplastic conditions |
| Malignant effusions |
Benign elements
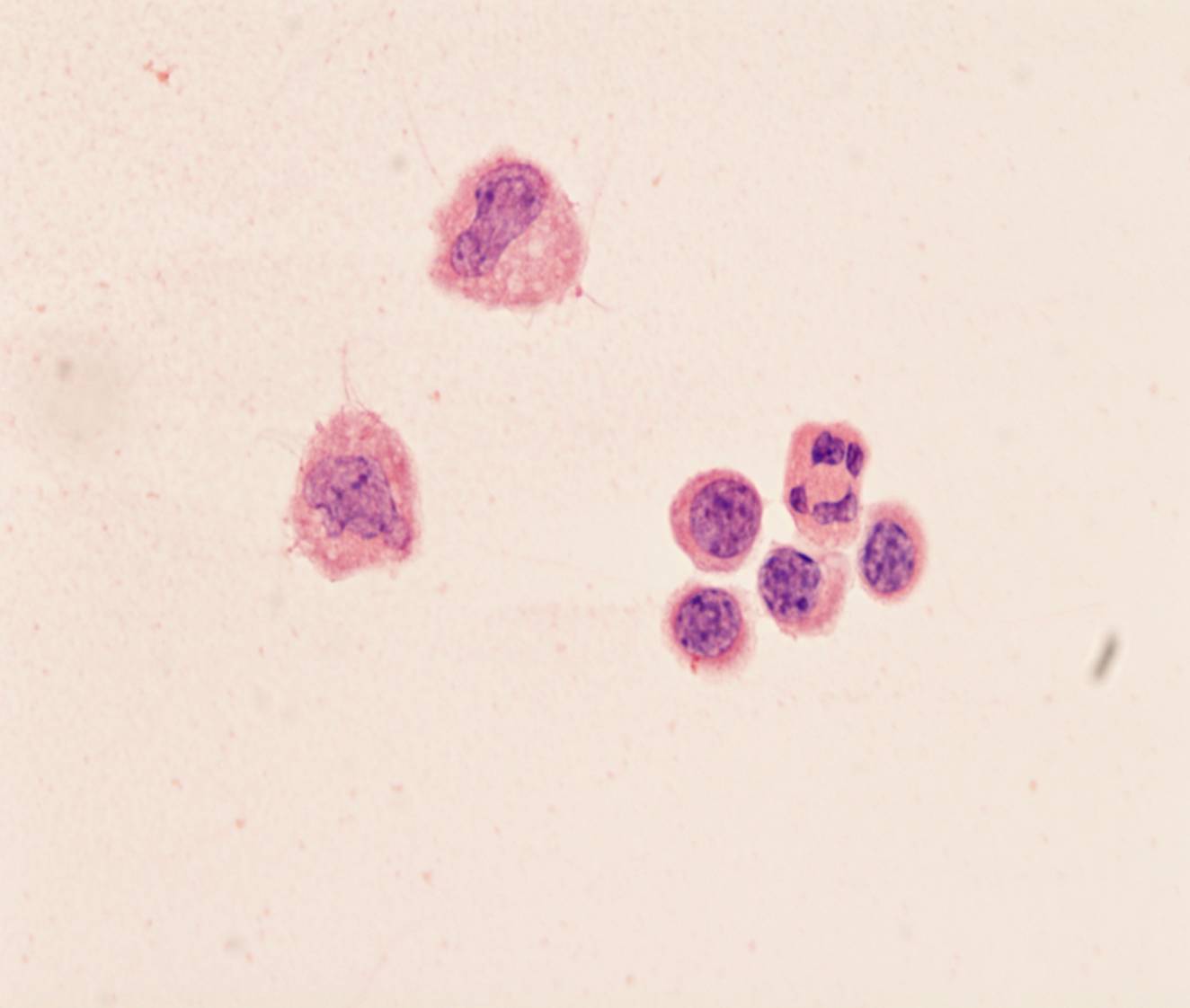
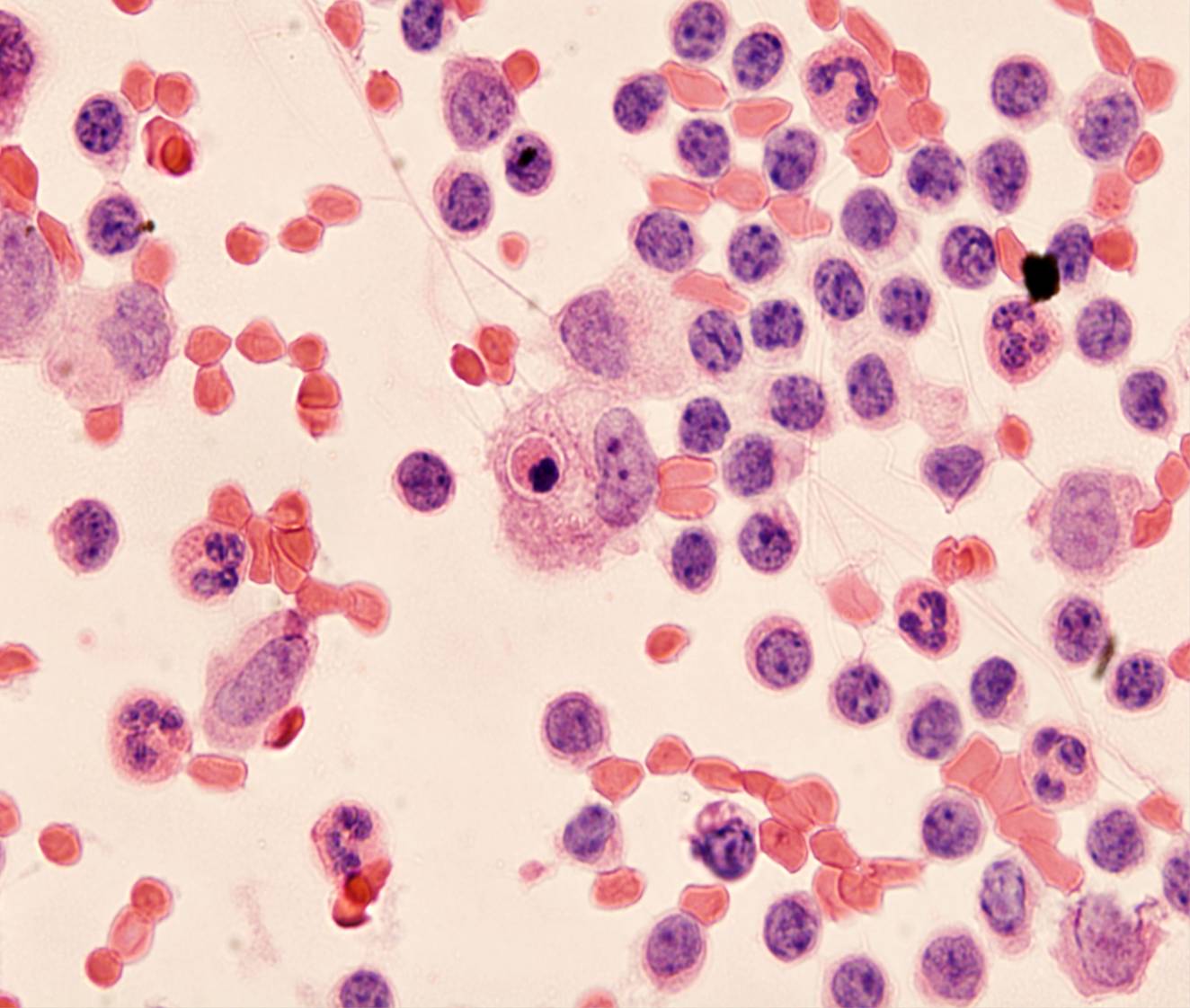
Benign effusions contain mesothelial cells, histiocytes and lymphocytes in varying proportions. Because some bleeding can often occur during specimen collection, red and white blood cells are common.
- Mesothelial cells
- Macrophages
- Lymphocytes
- Neutrophils
- Eosinophils
- Plasma cells
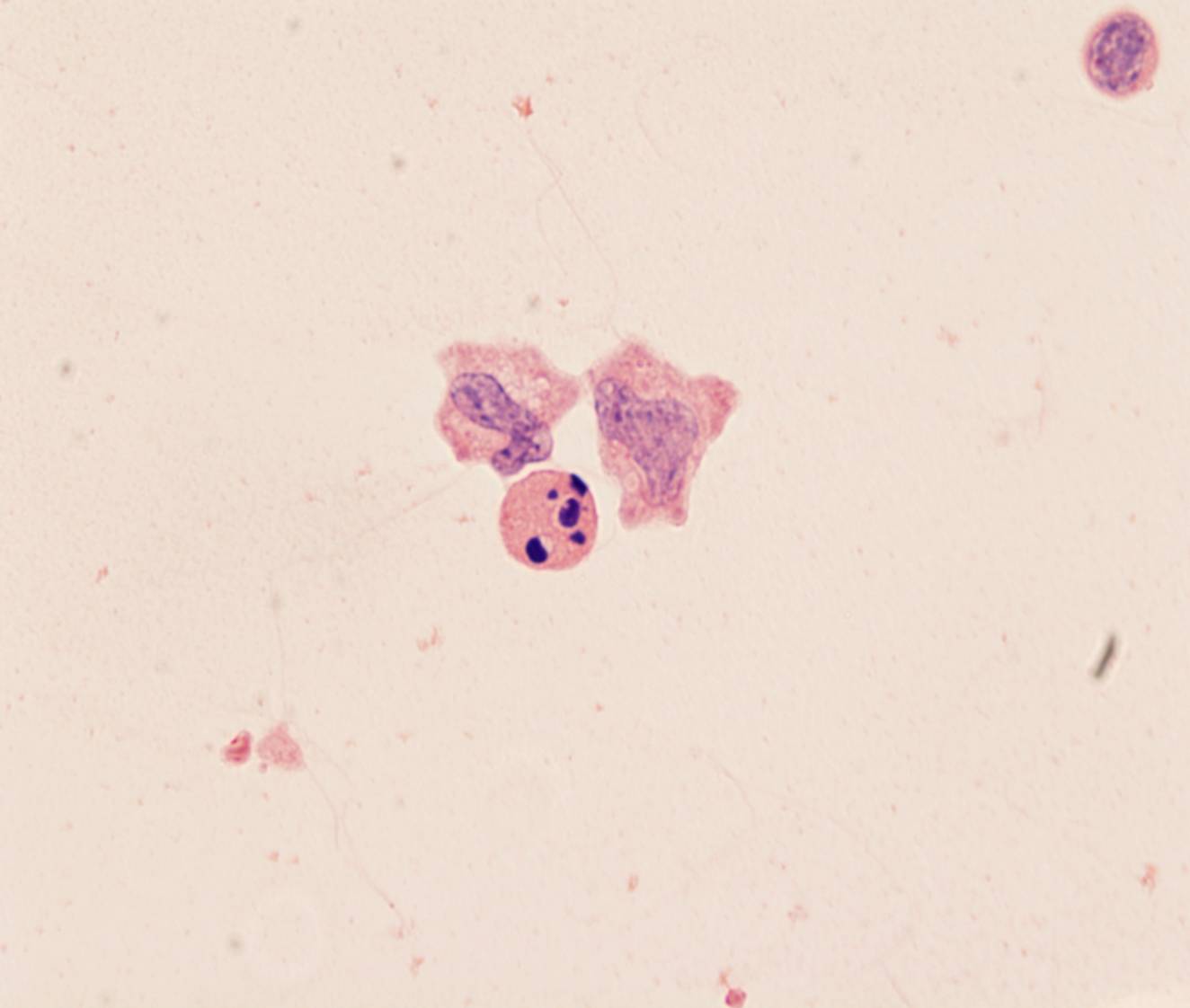
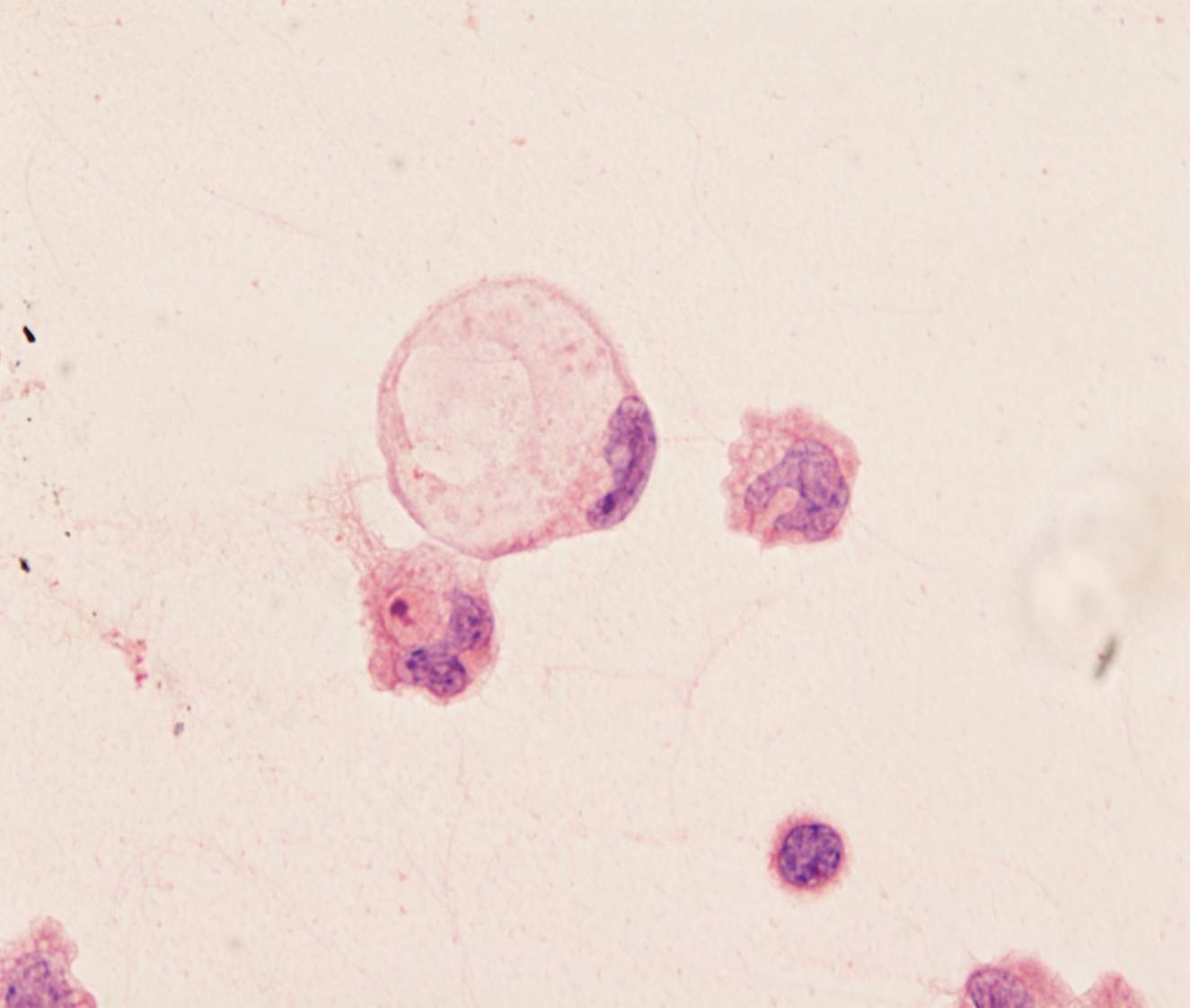
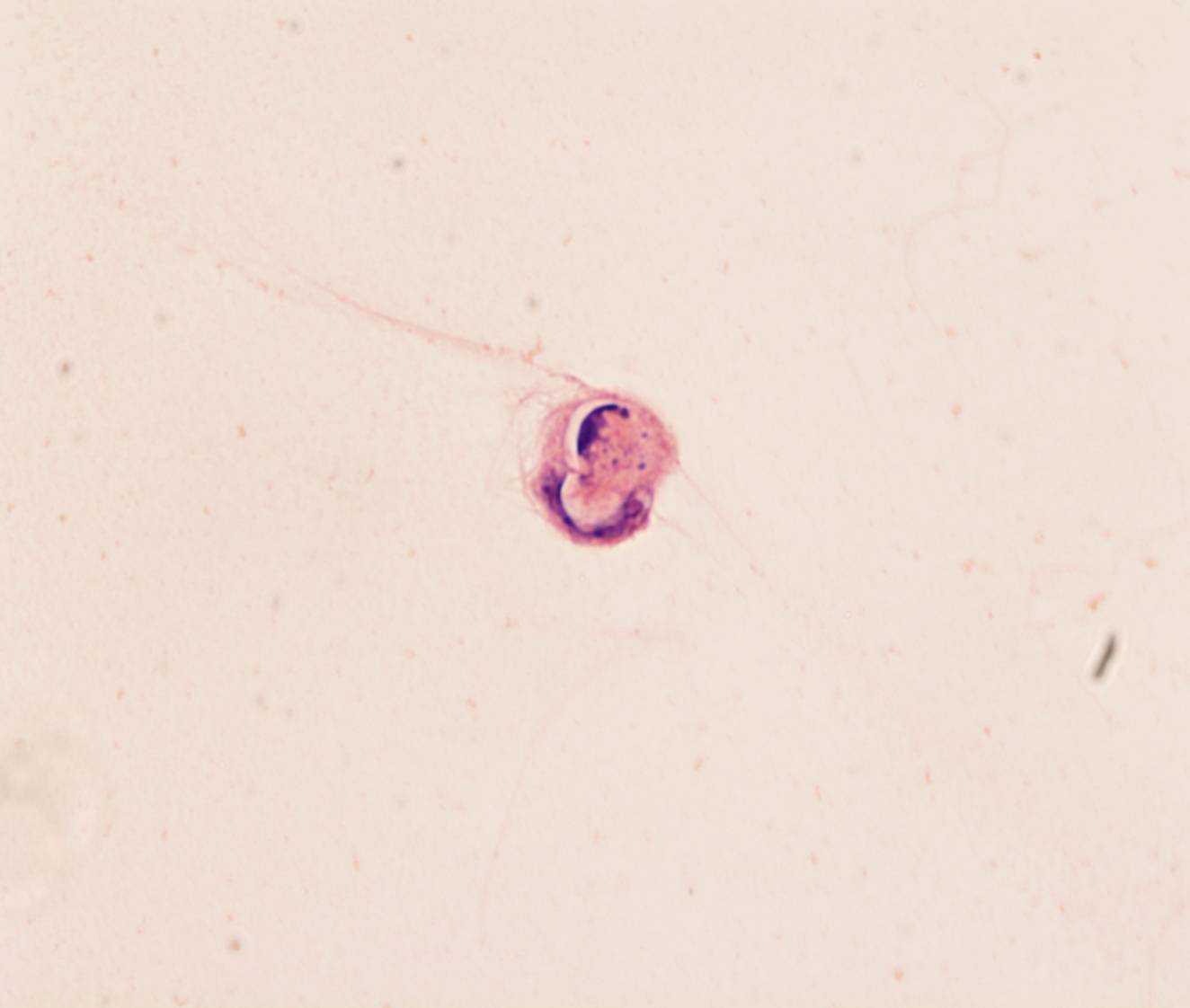
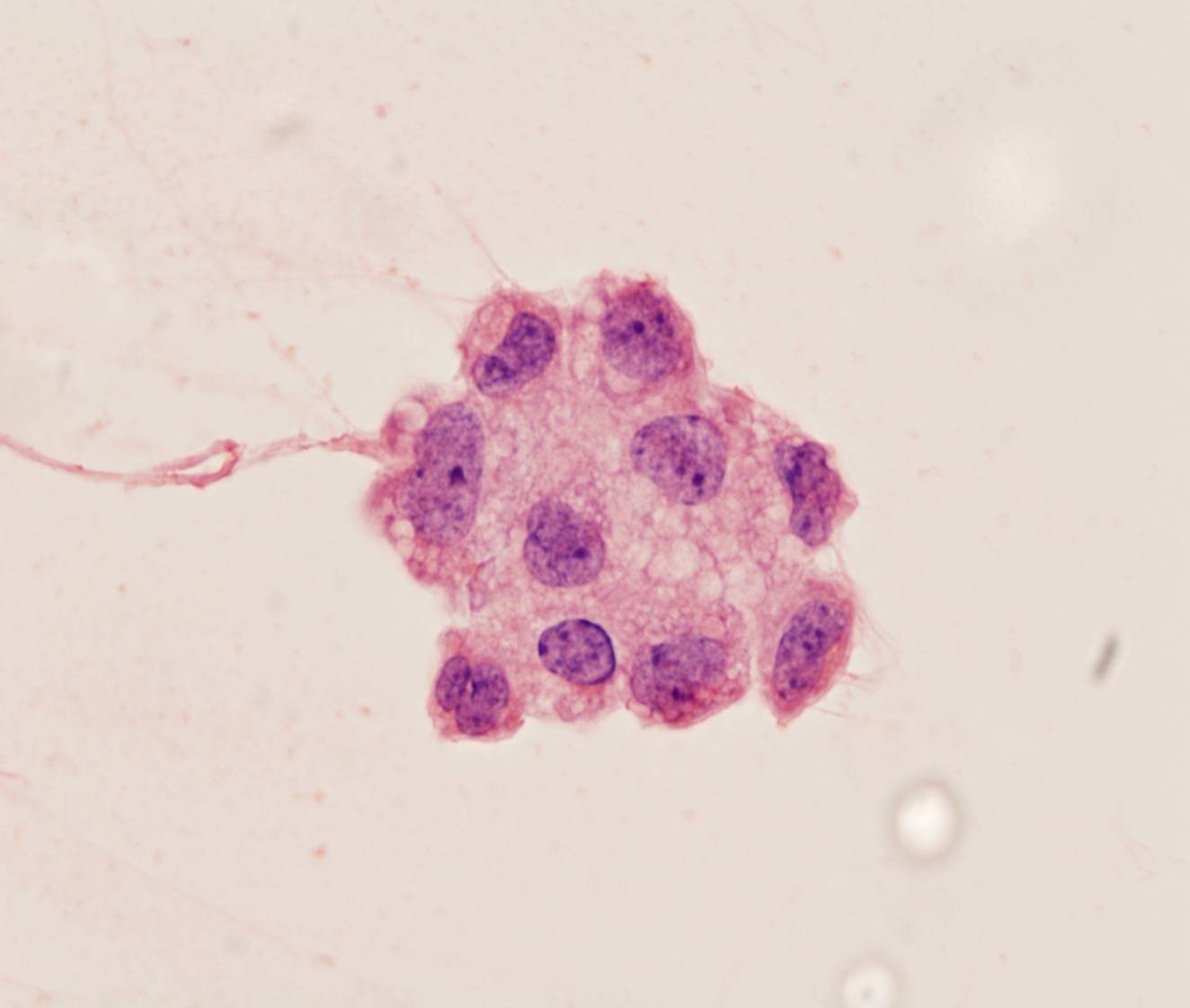
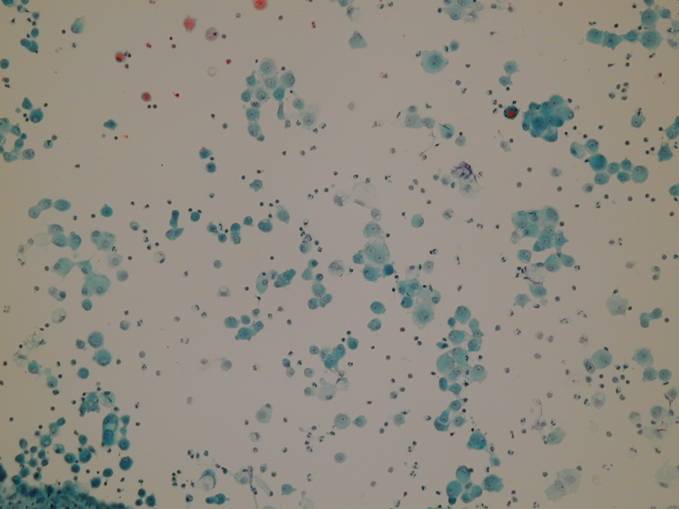
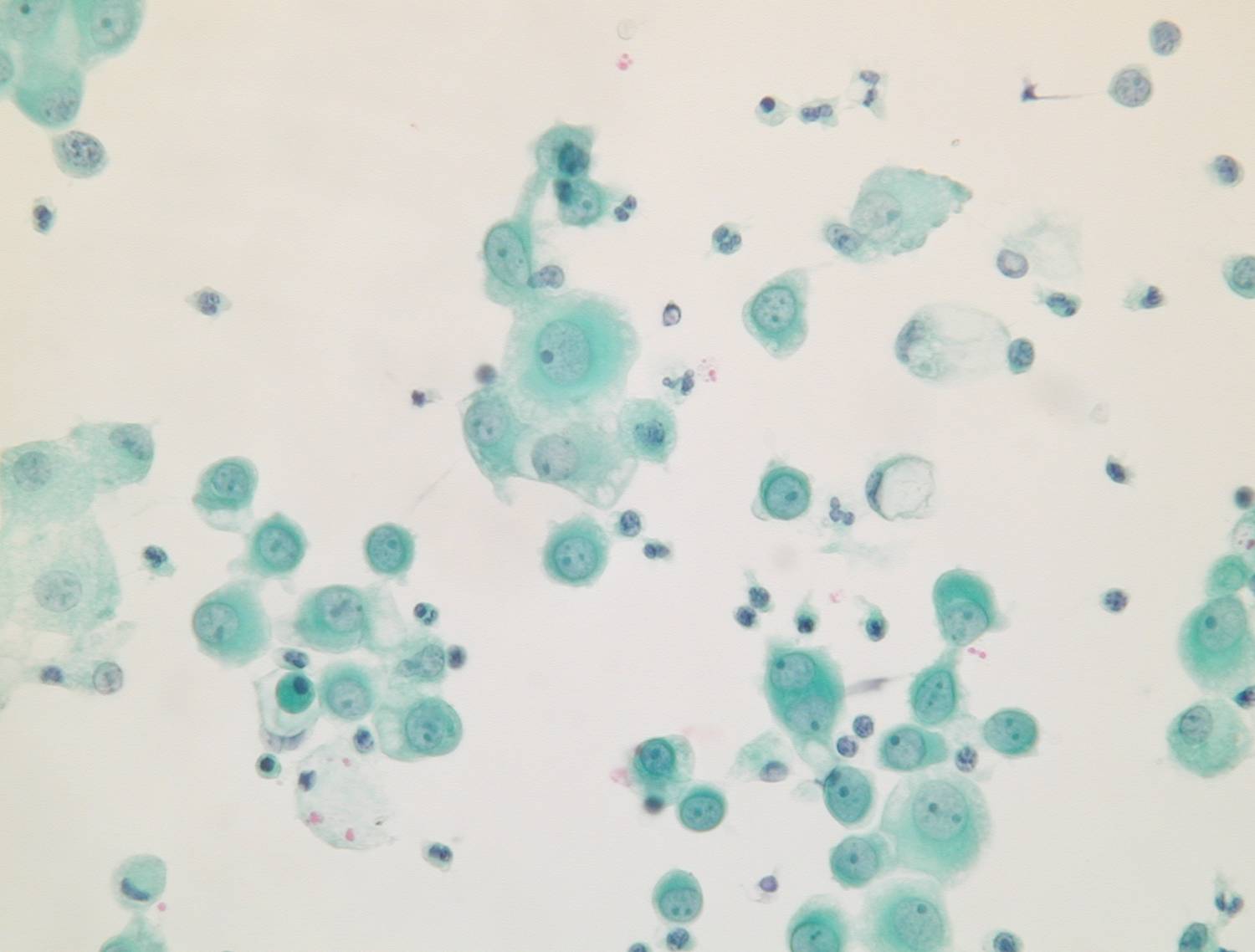
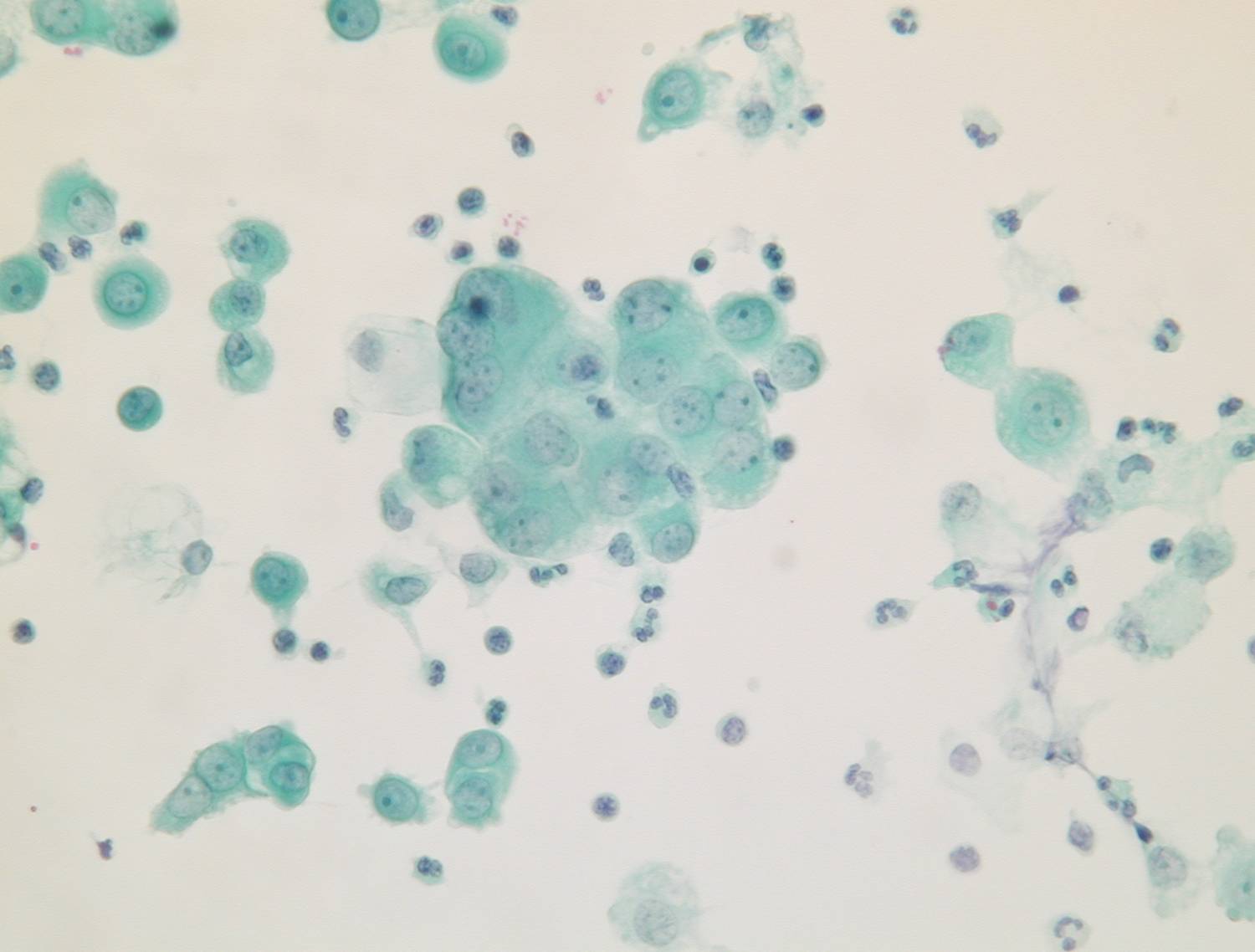
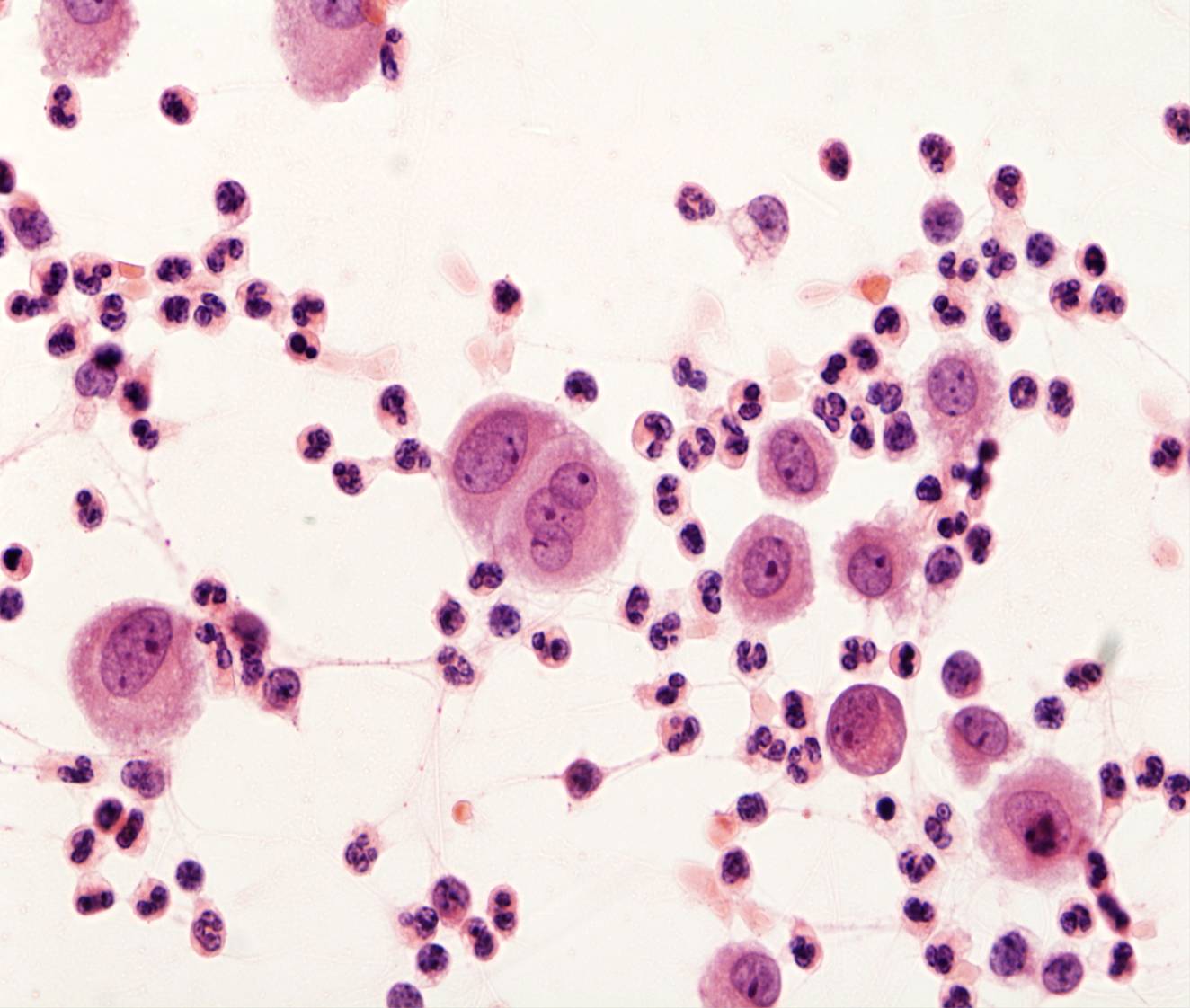
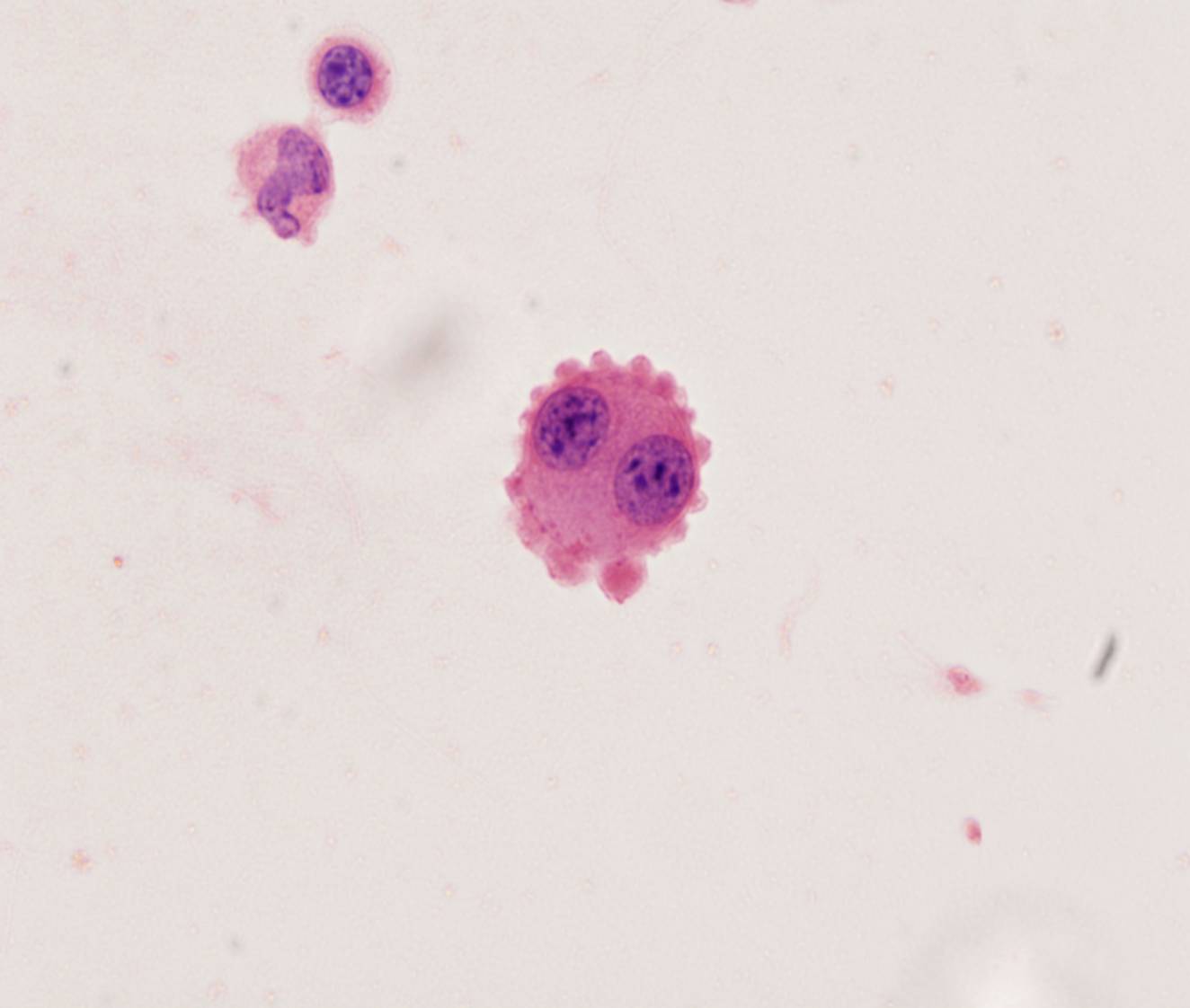
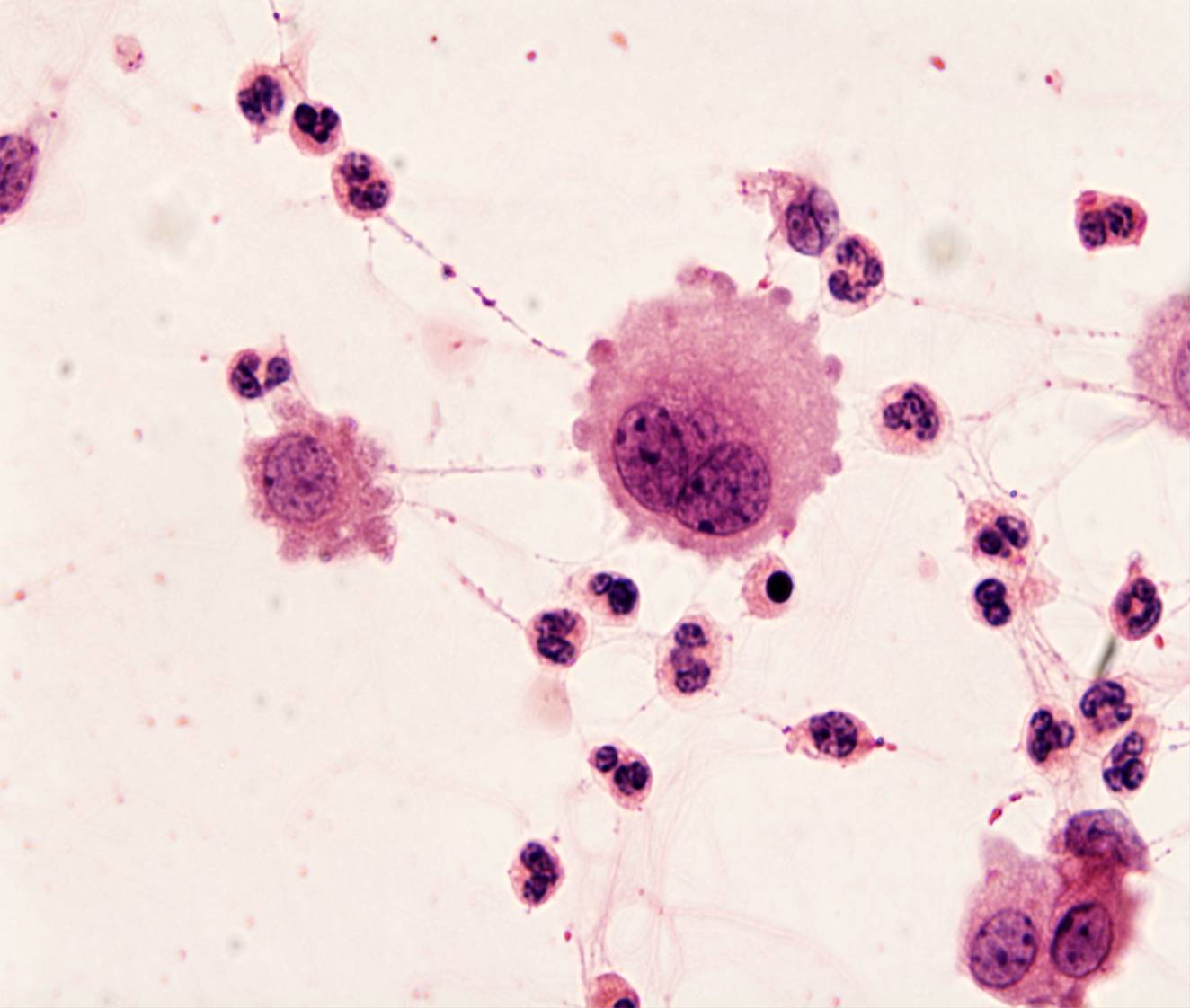
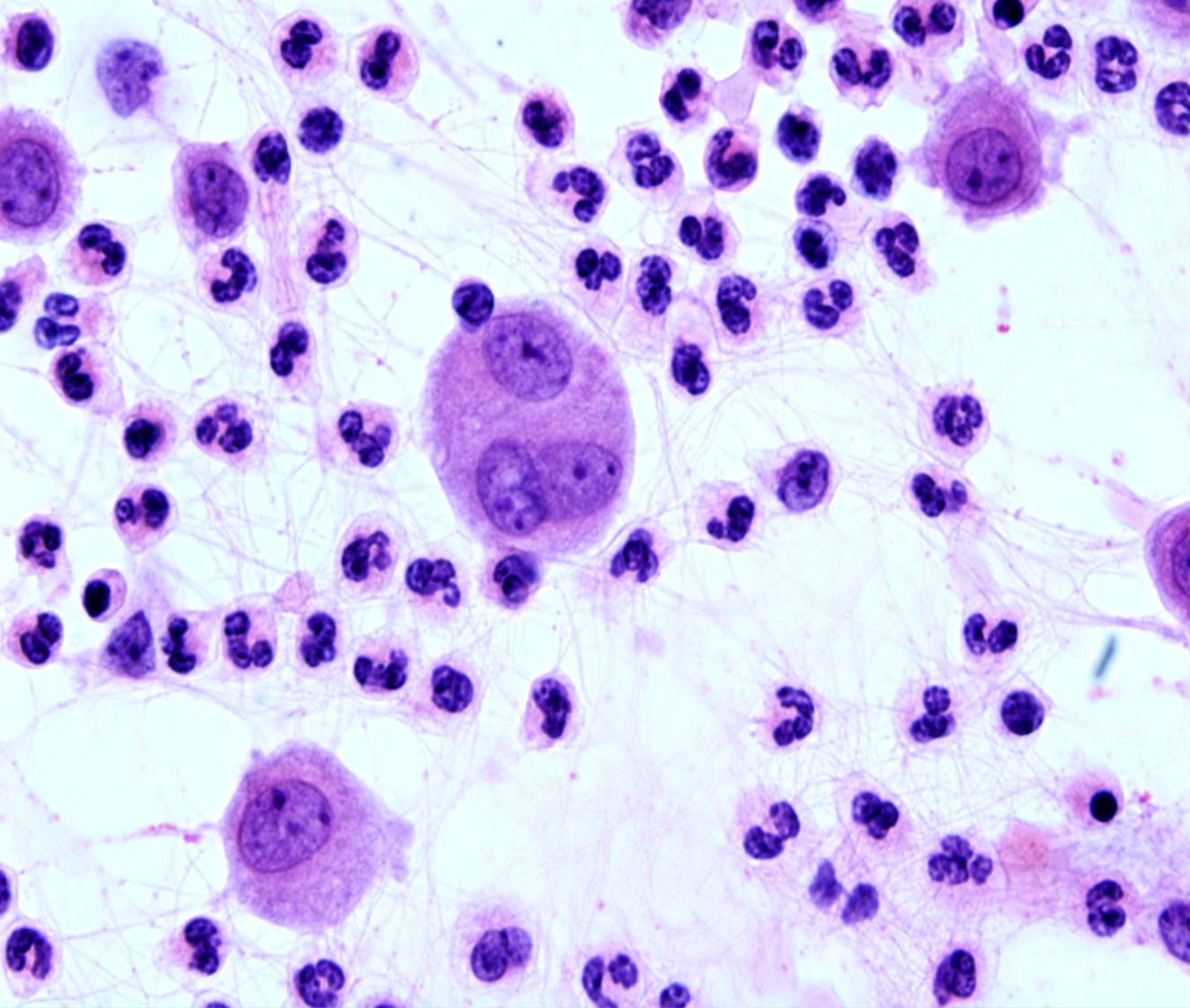
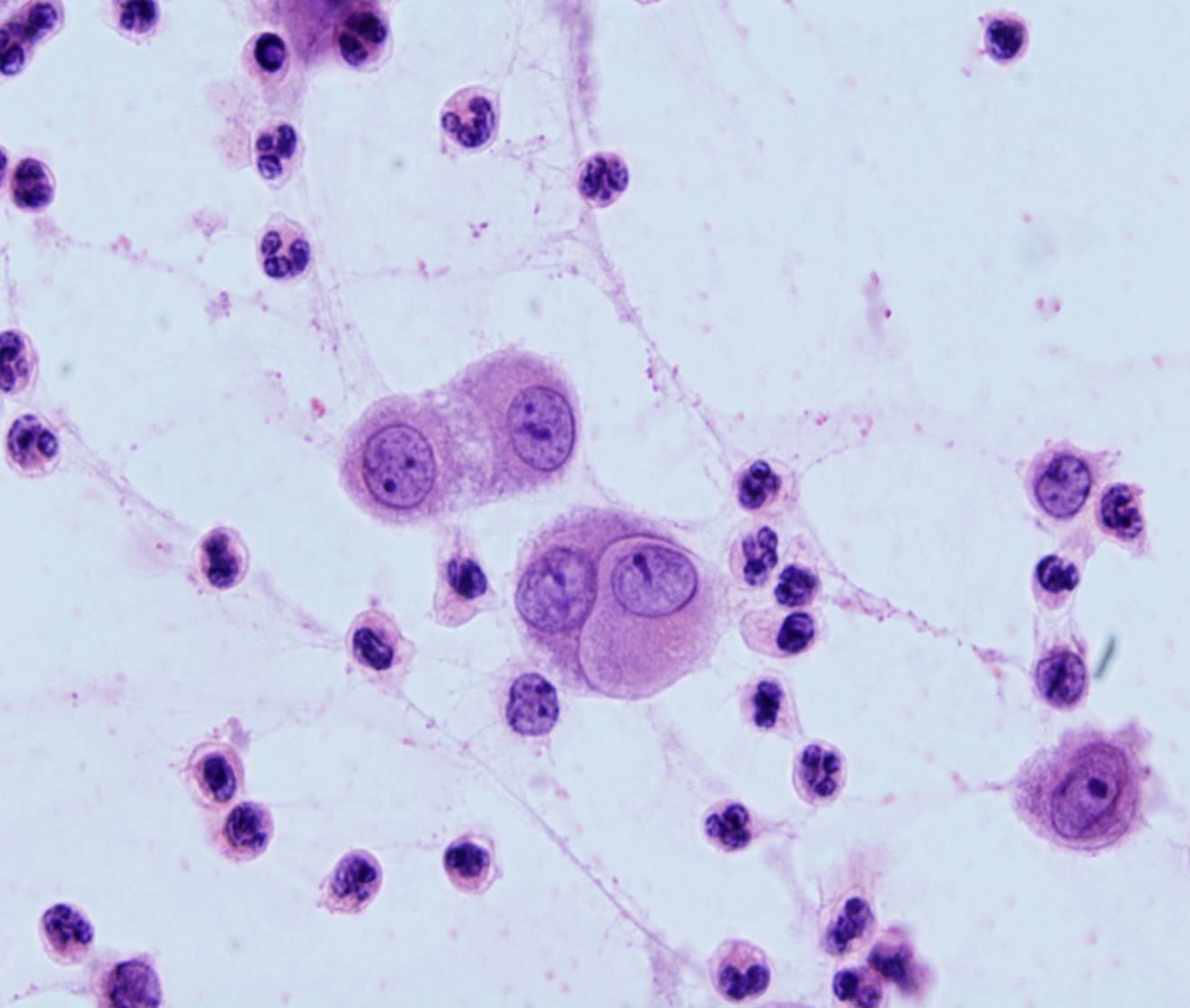
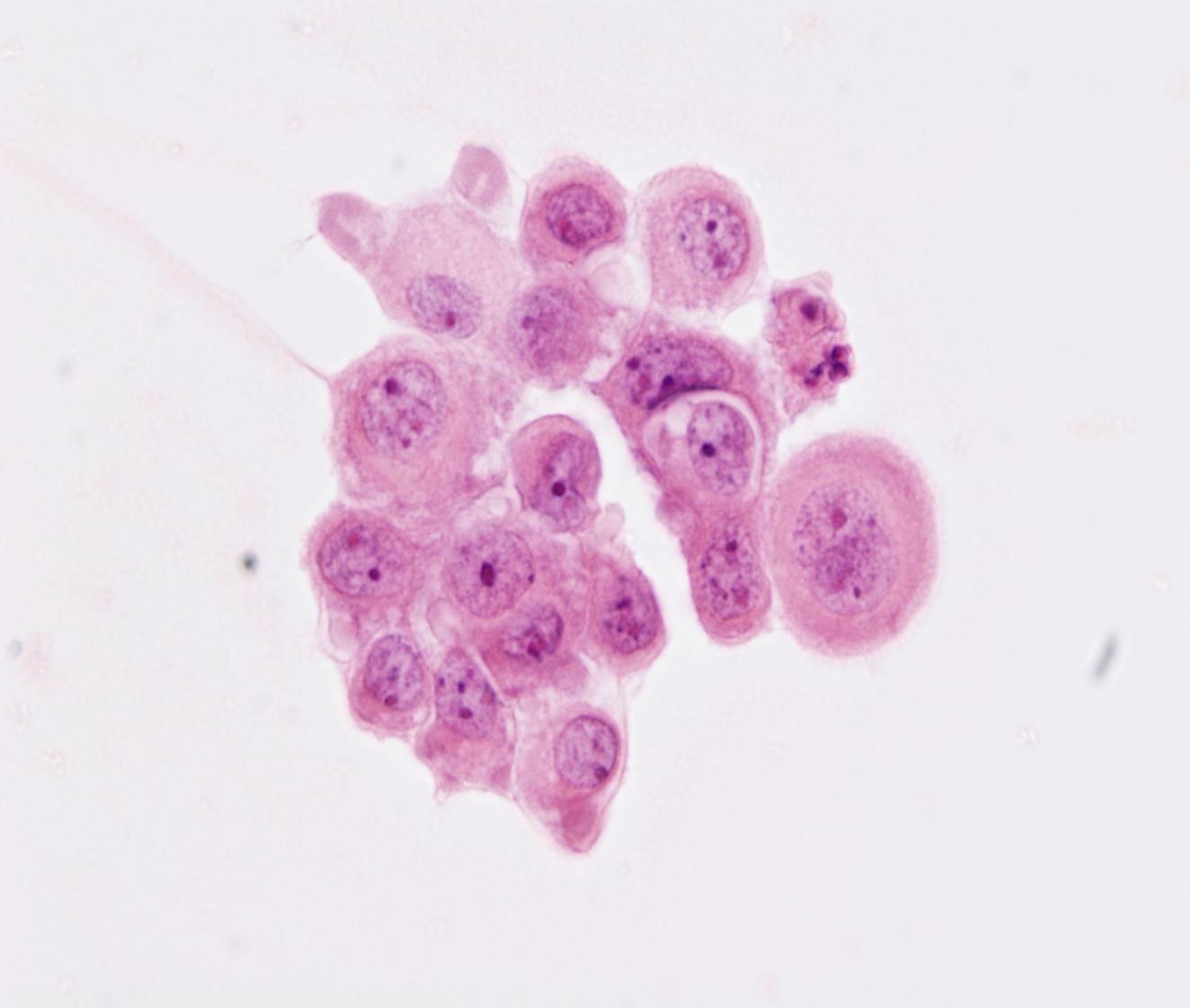
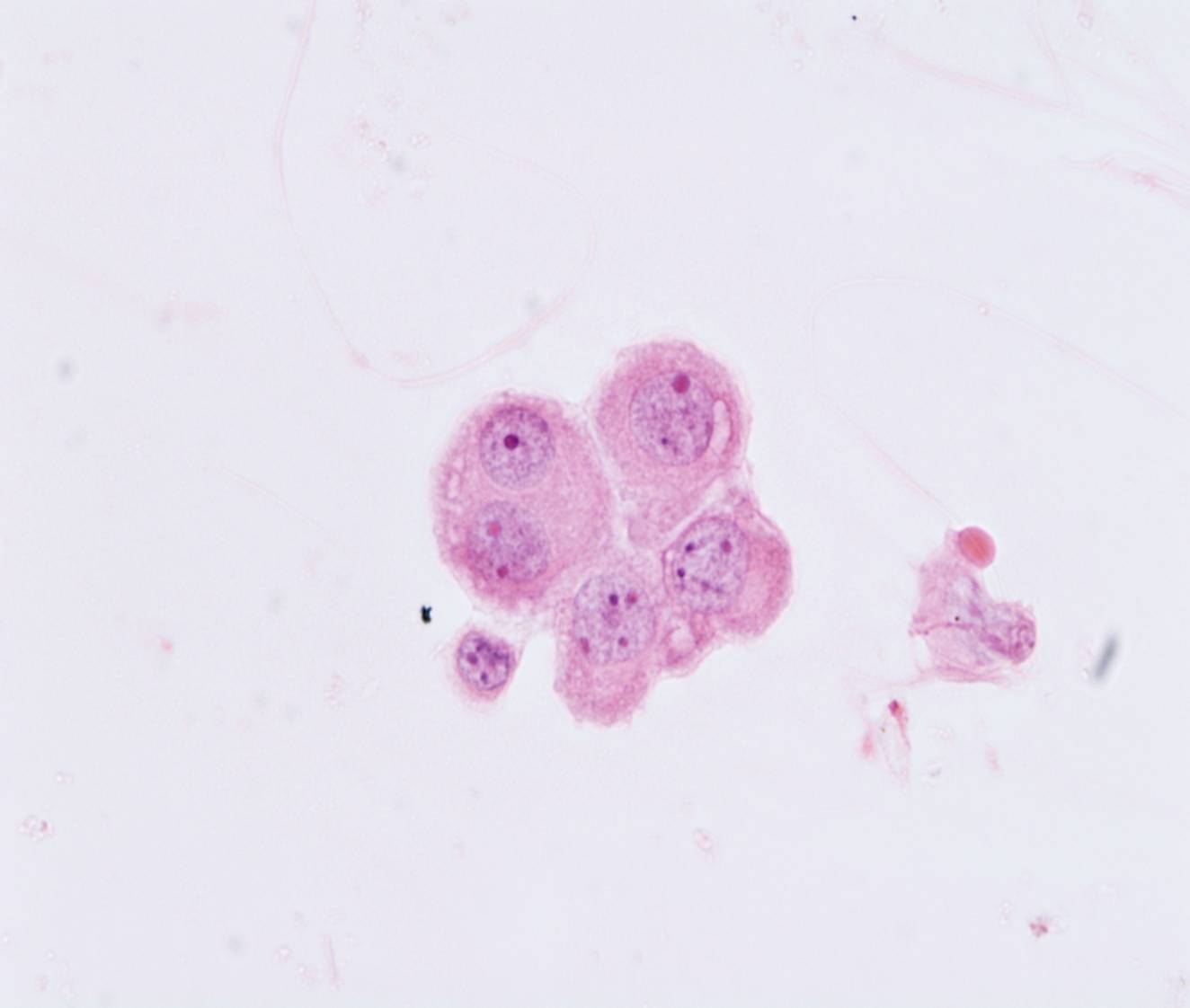
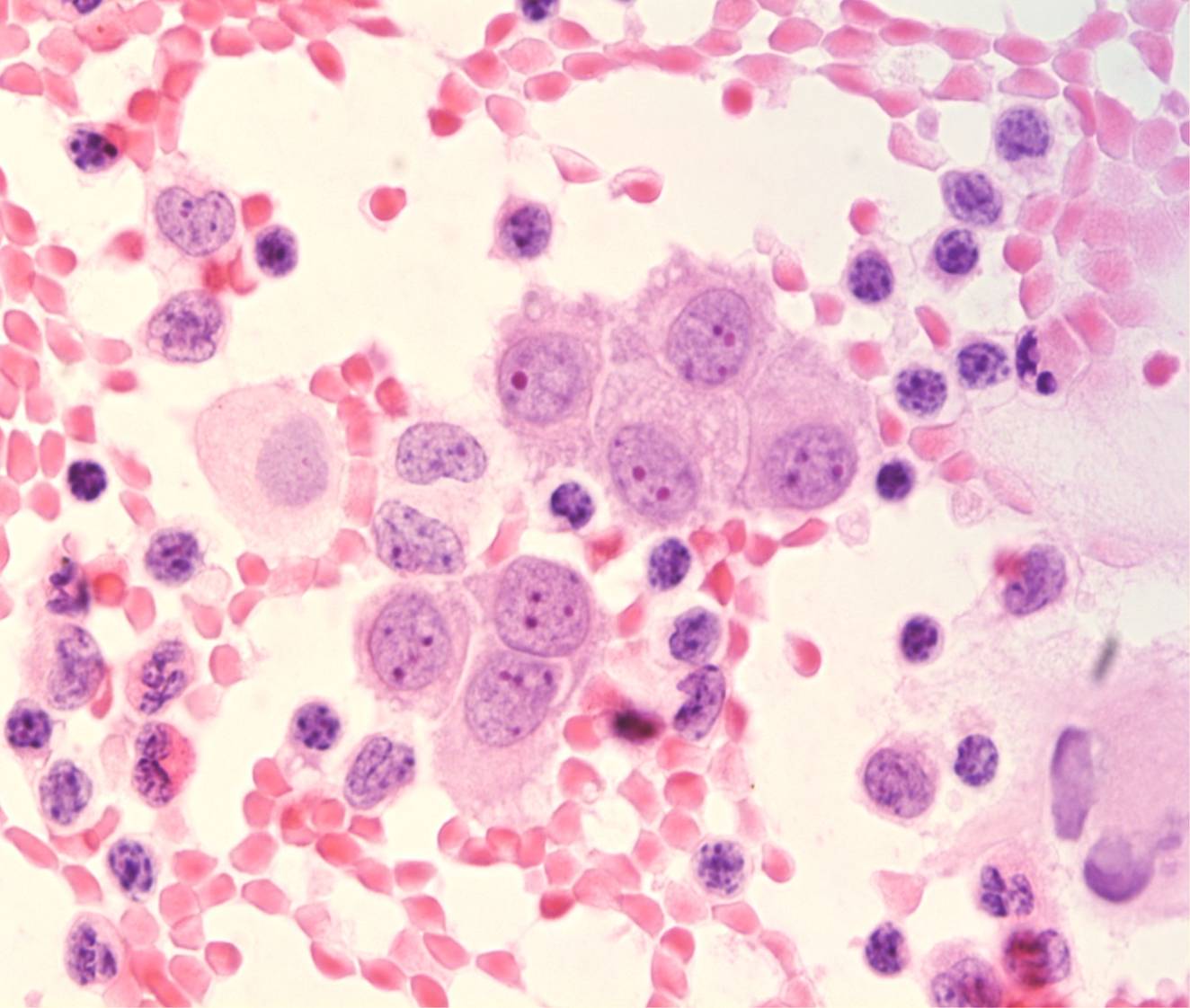
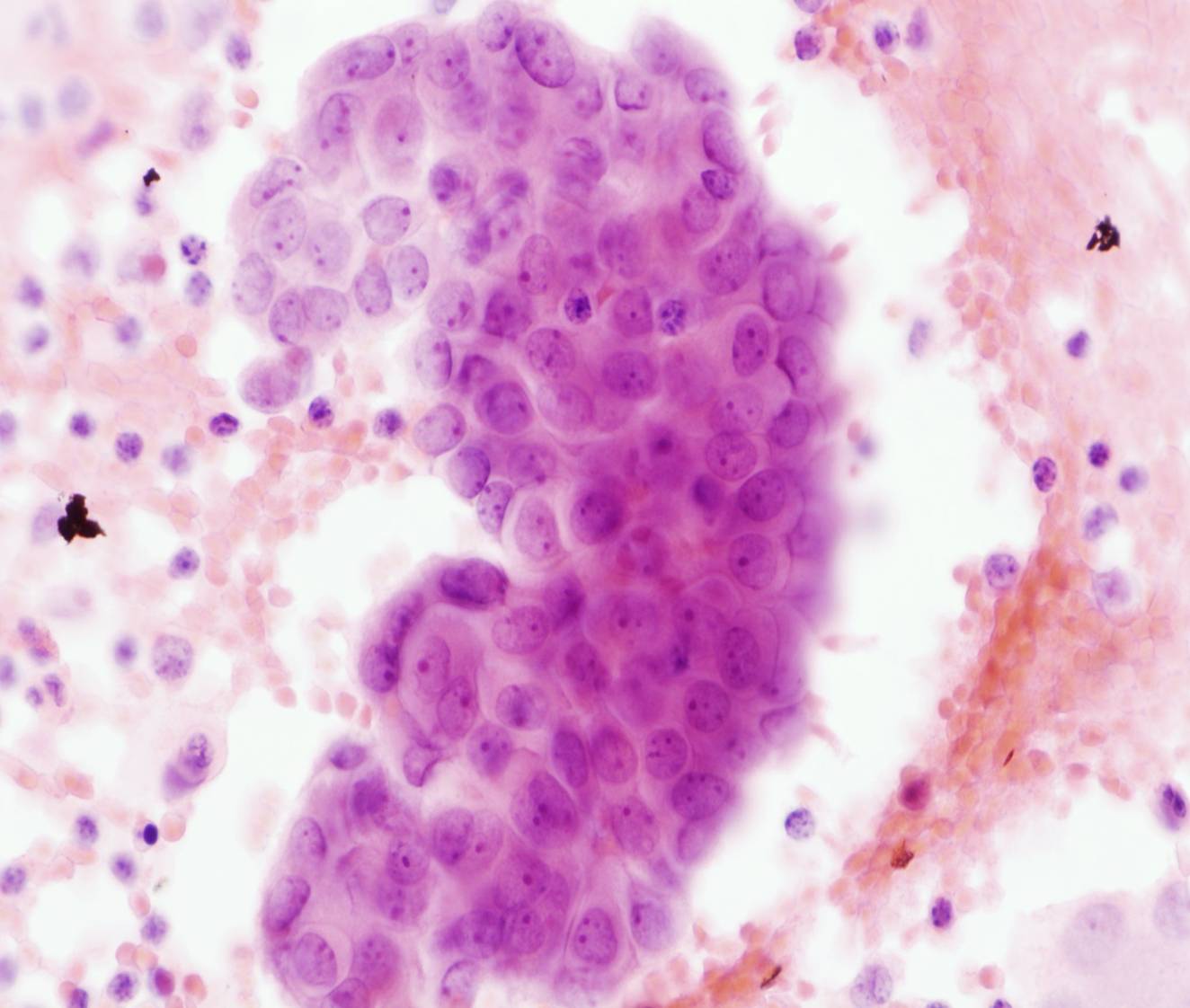
Mesothelial cells
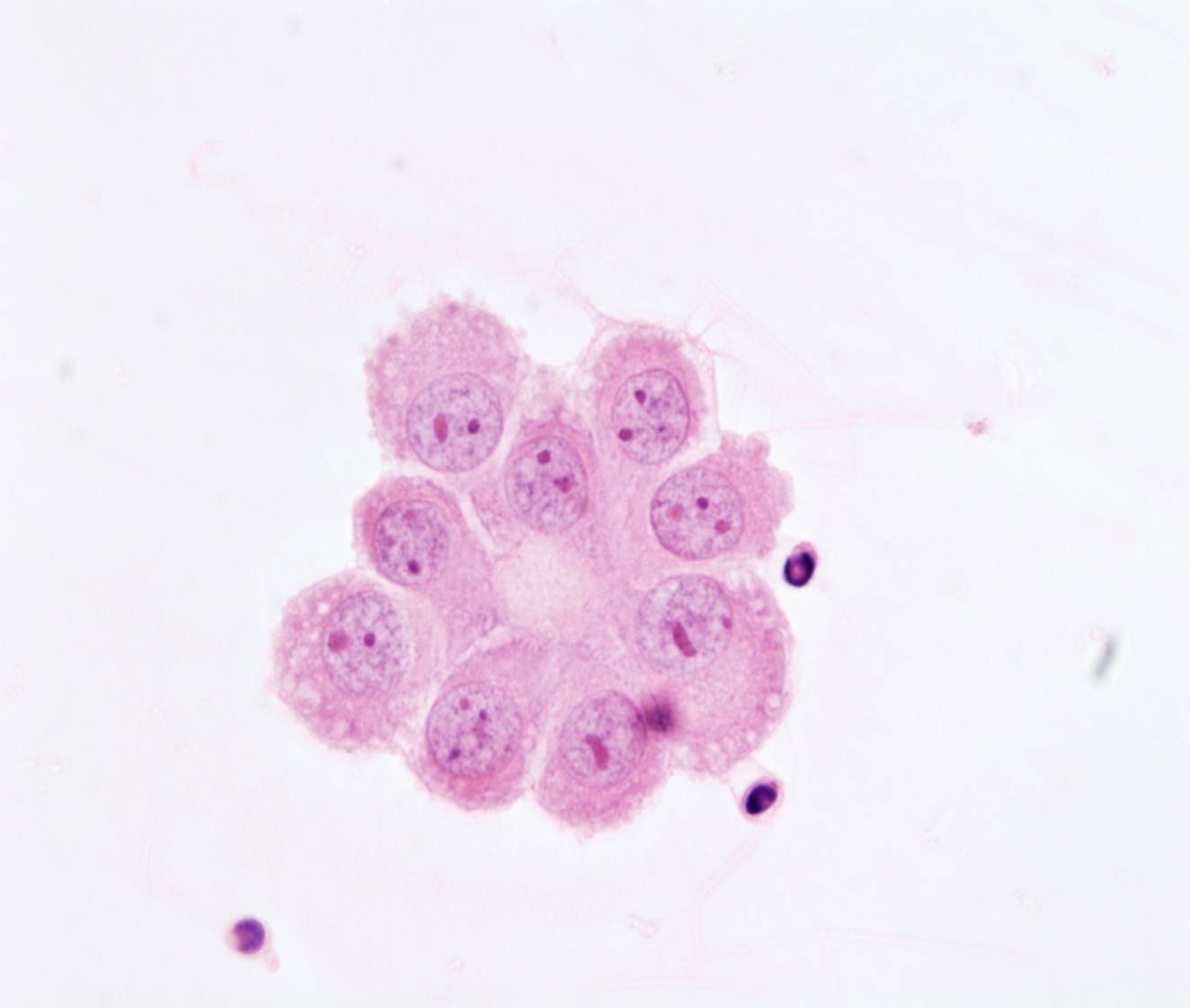
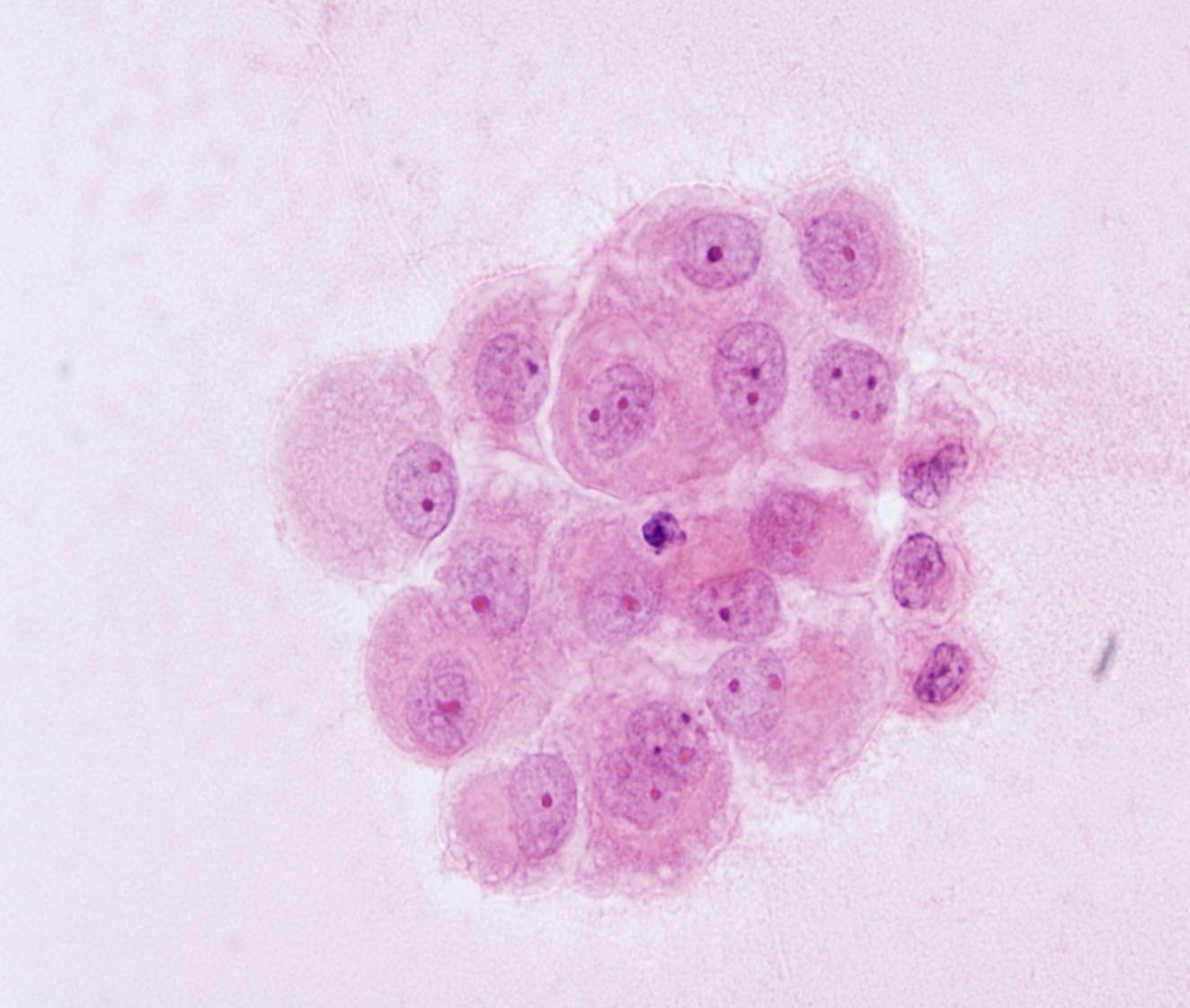
- Usually dispersed as isolated cells
- Occasional sheets or small clusters with ‘windows’
- Round cells
- Round nucleus, single nucleolus
- Dense cytoplasm with clear outer rim (‘lacy skirt’)
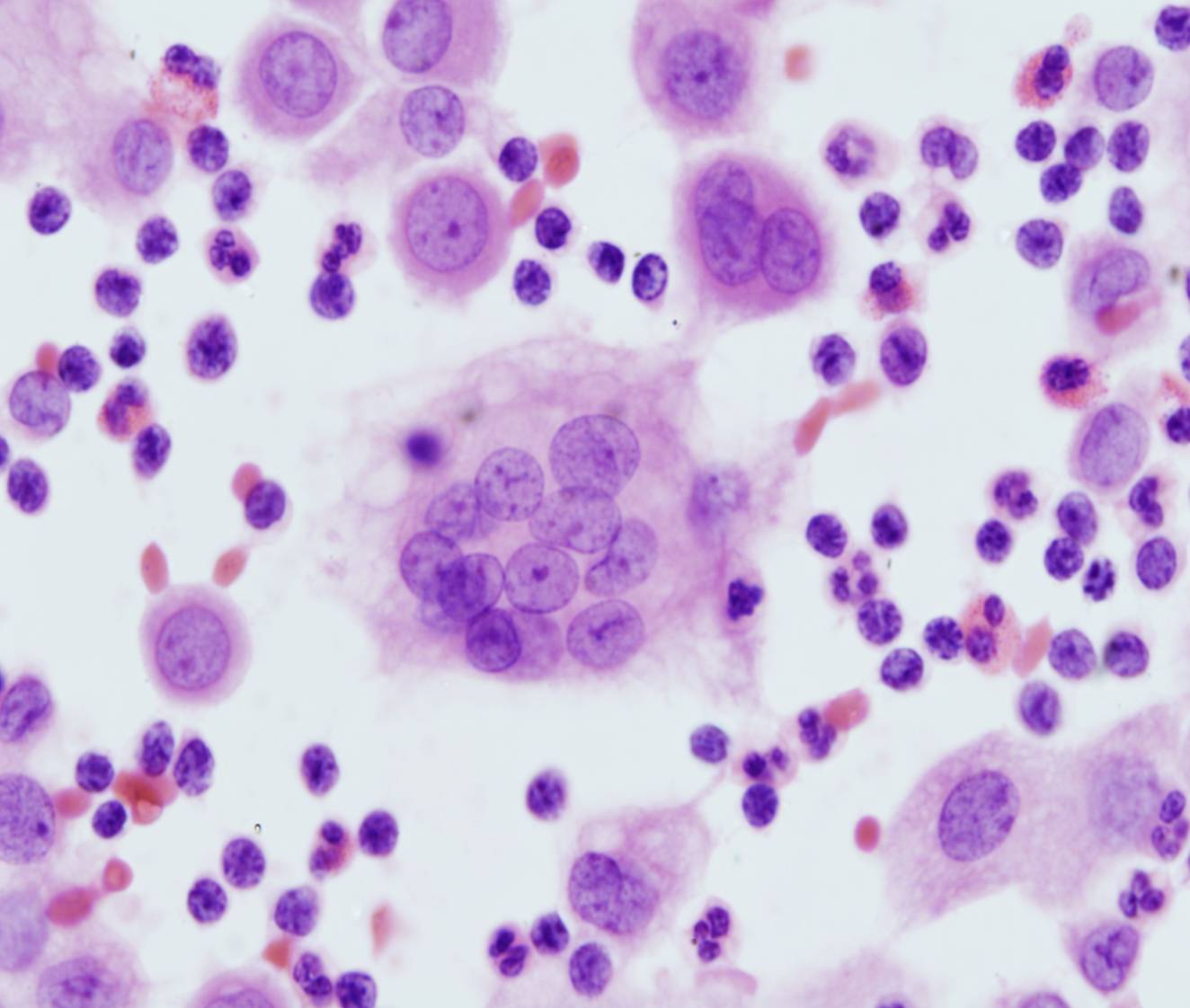
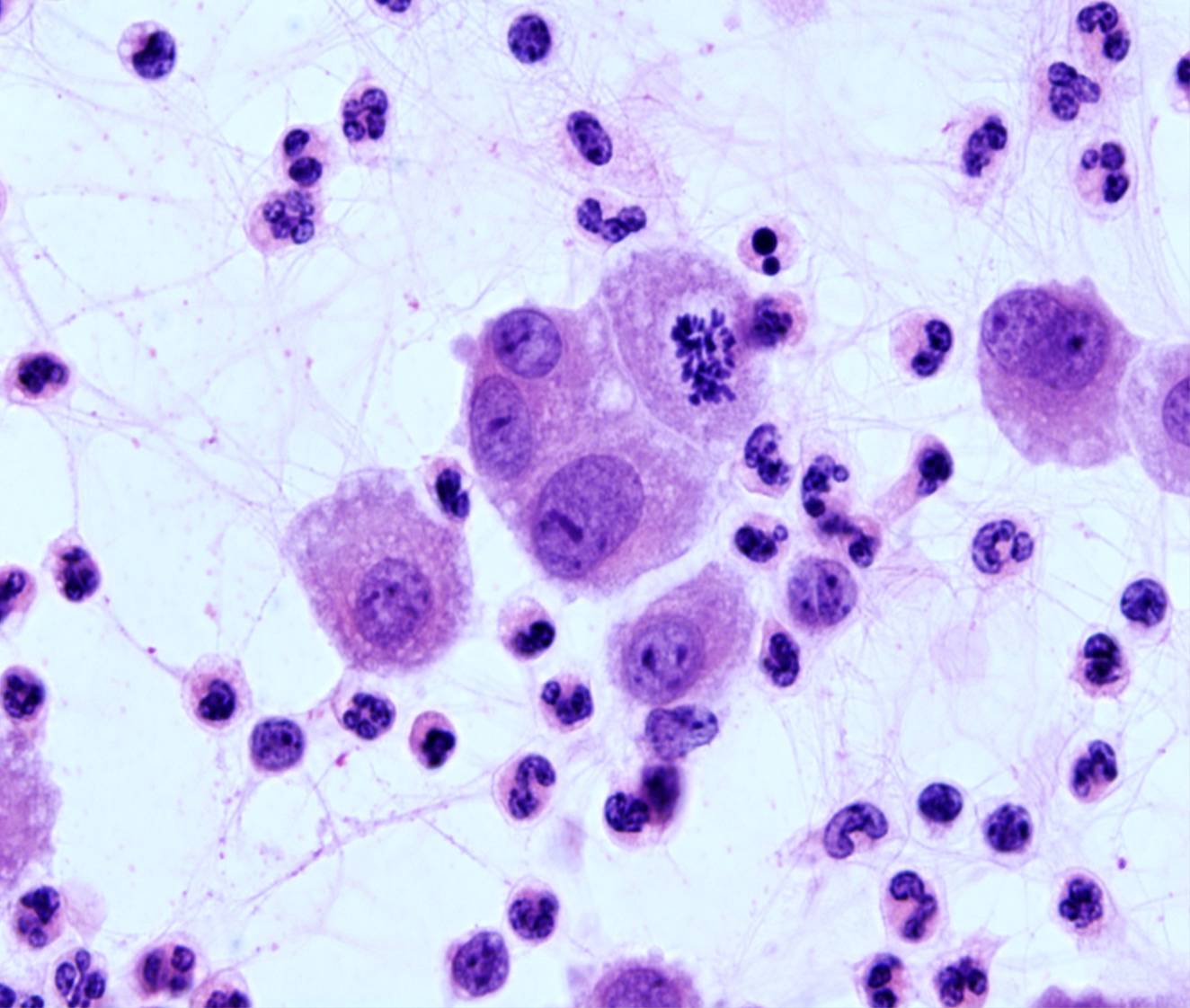
- Occasional giant, multinucleated cells
Mesothelial cells may be sparse or numerous. Binucleation and multinucleation are common and mitoses can be seen in benign effusions. The dense cytoplasm reflects the abundance of tonofilaments, and the clear outer rim (‘lacy skirt’ or ‘halo’) corresponds to long, slender, branching microvilli. The cells sometimes have cytoplasmic vacuoles. Two or more mesothelial cells in groups are often separated by a narrow clear zone or ‘window’.
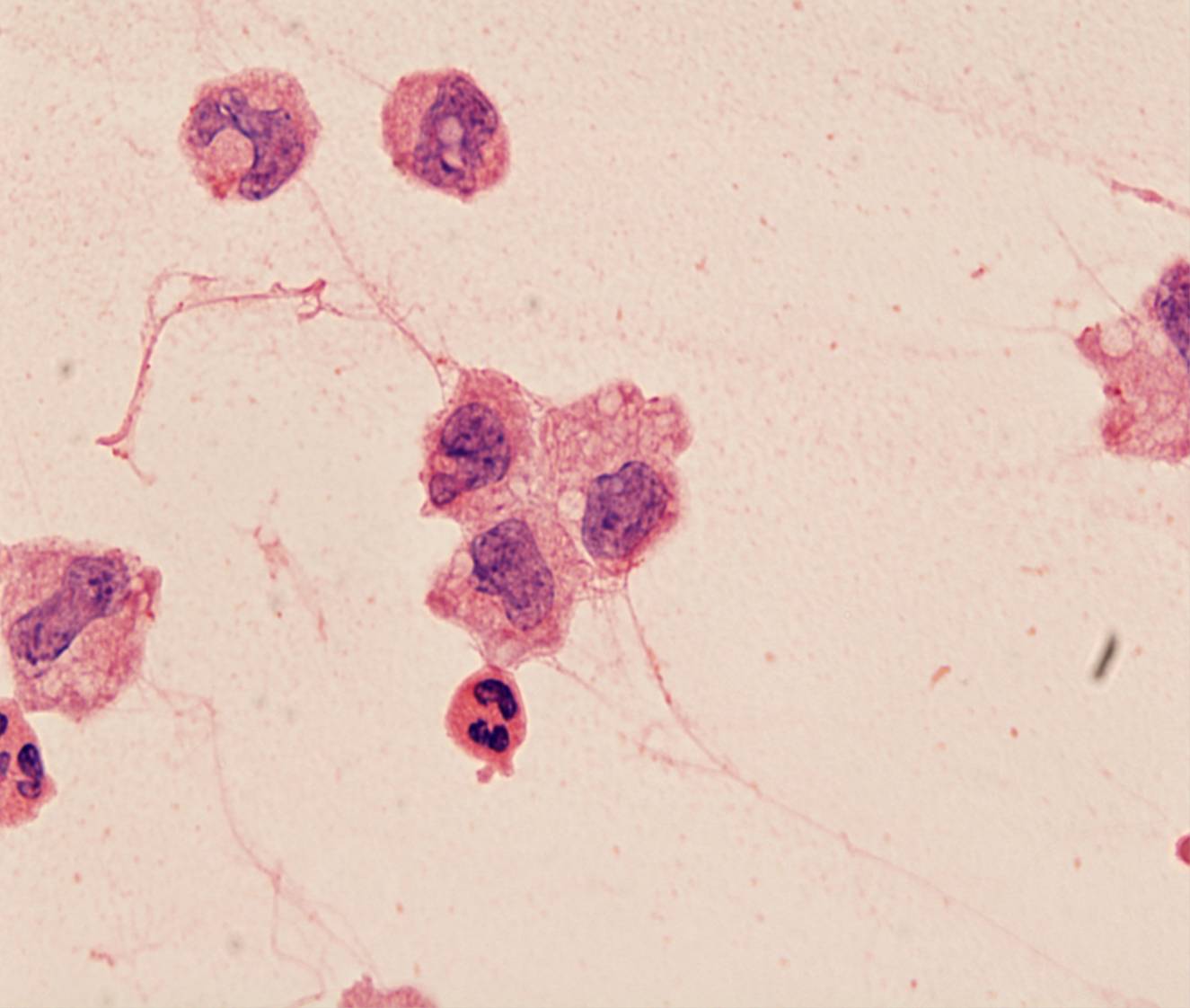
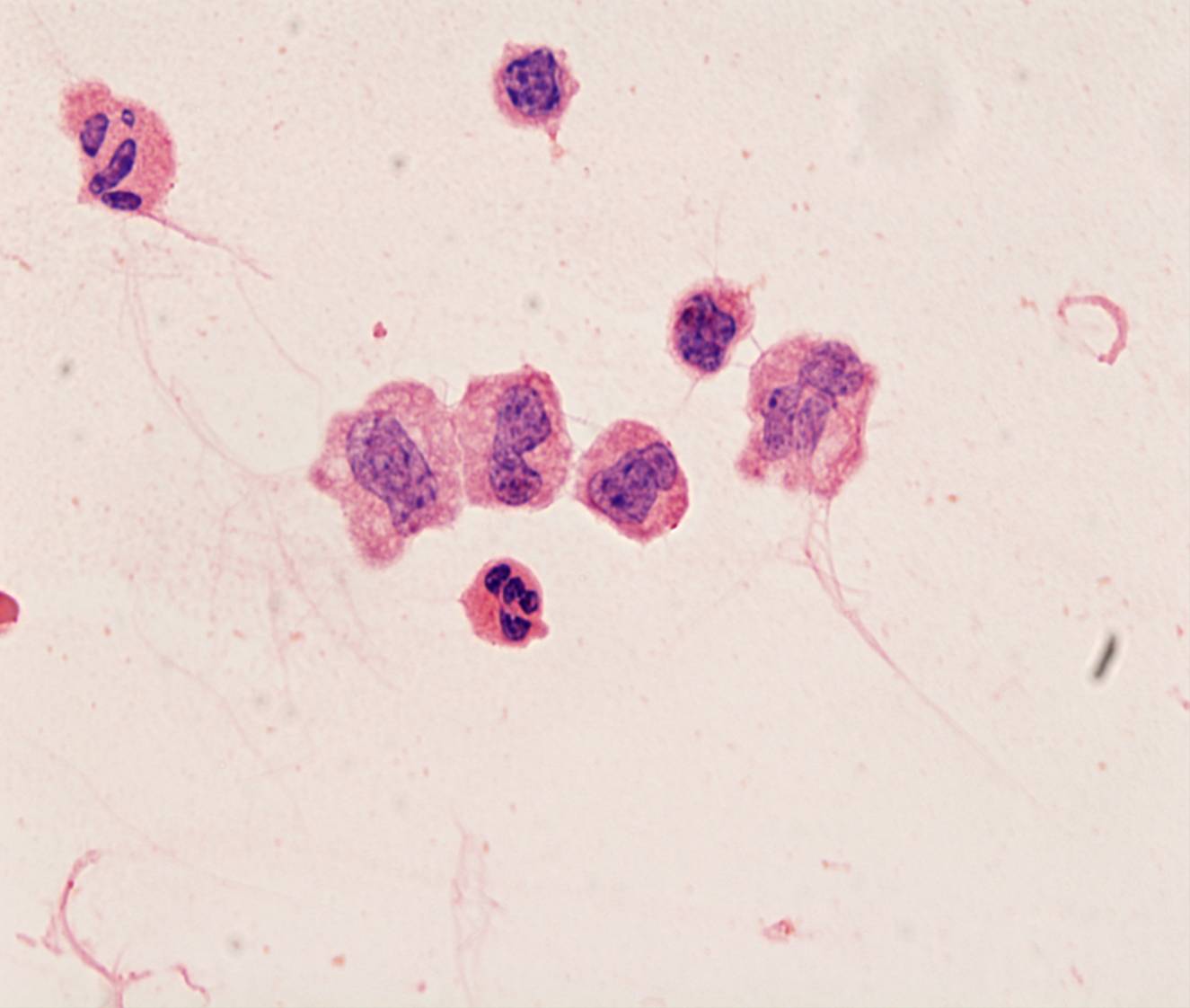
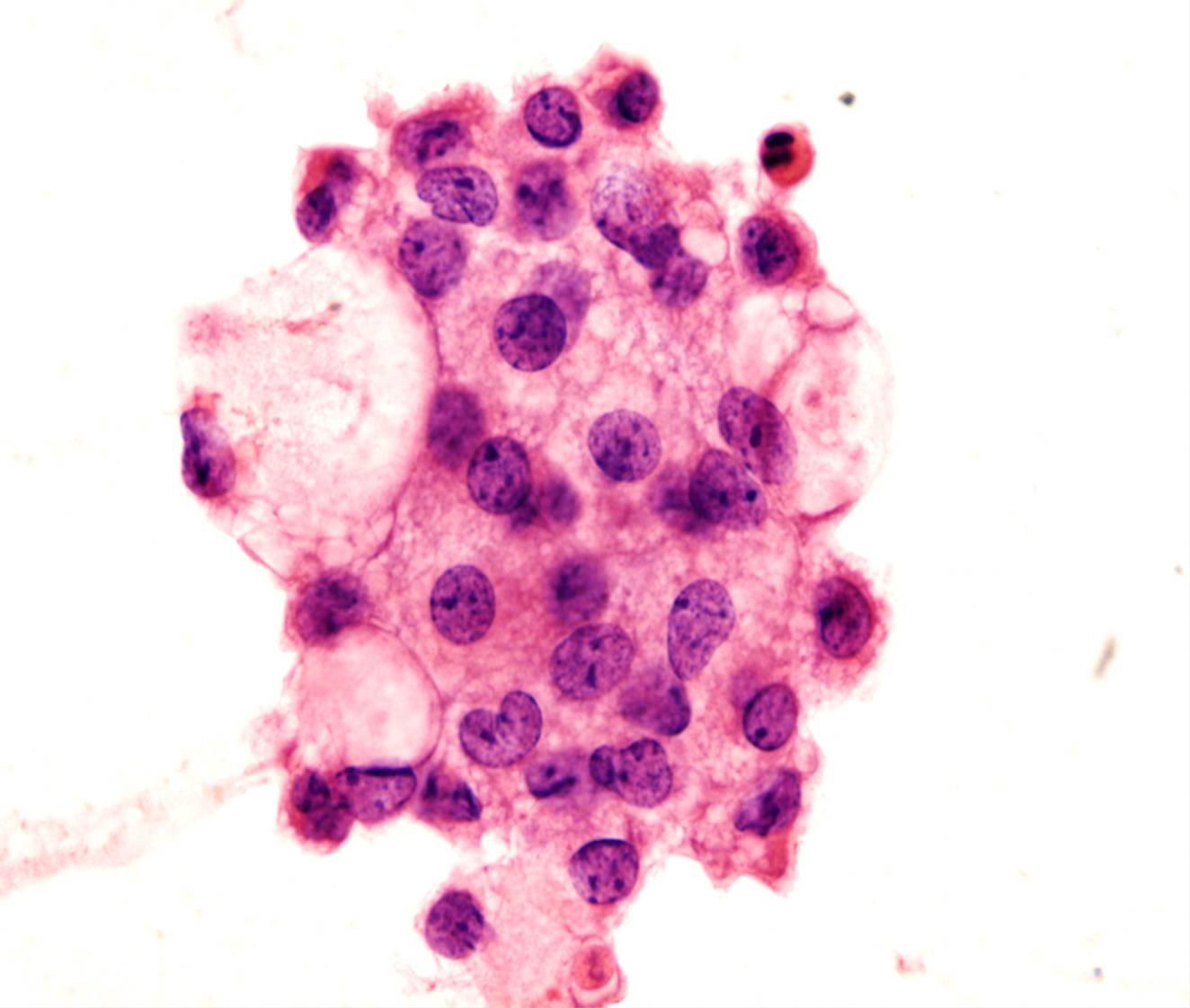
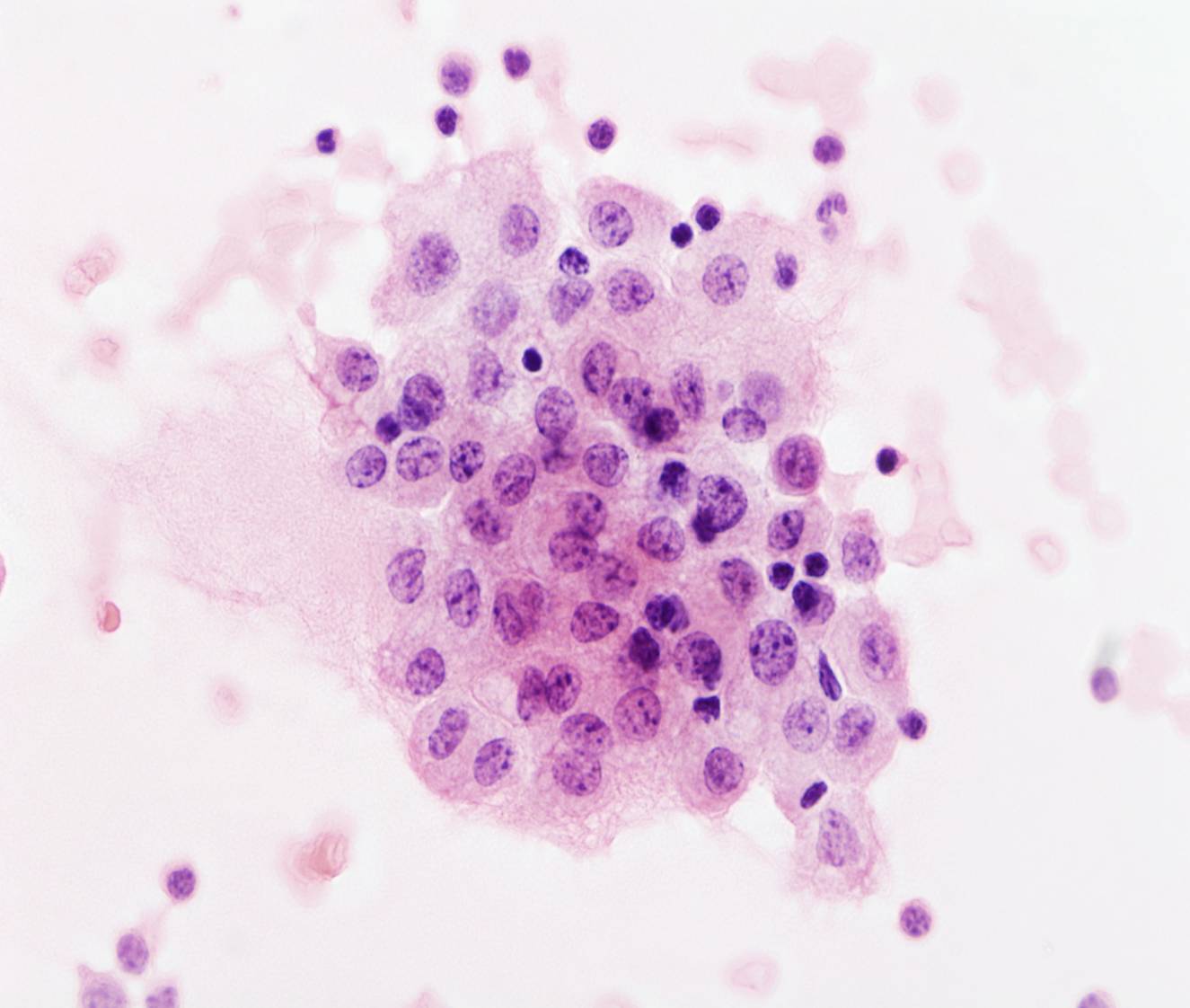
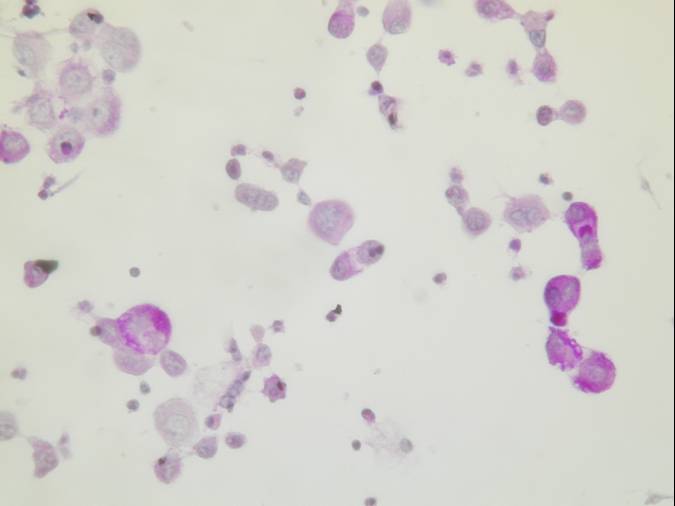
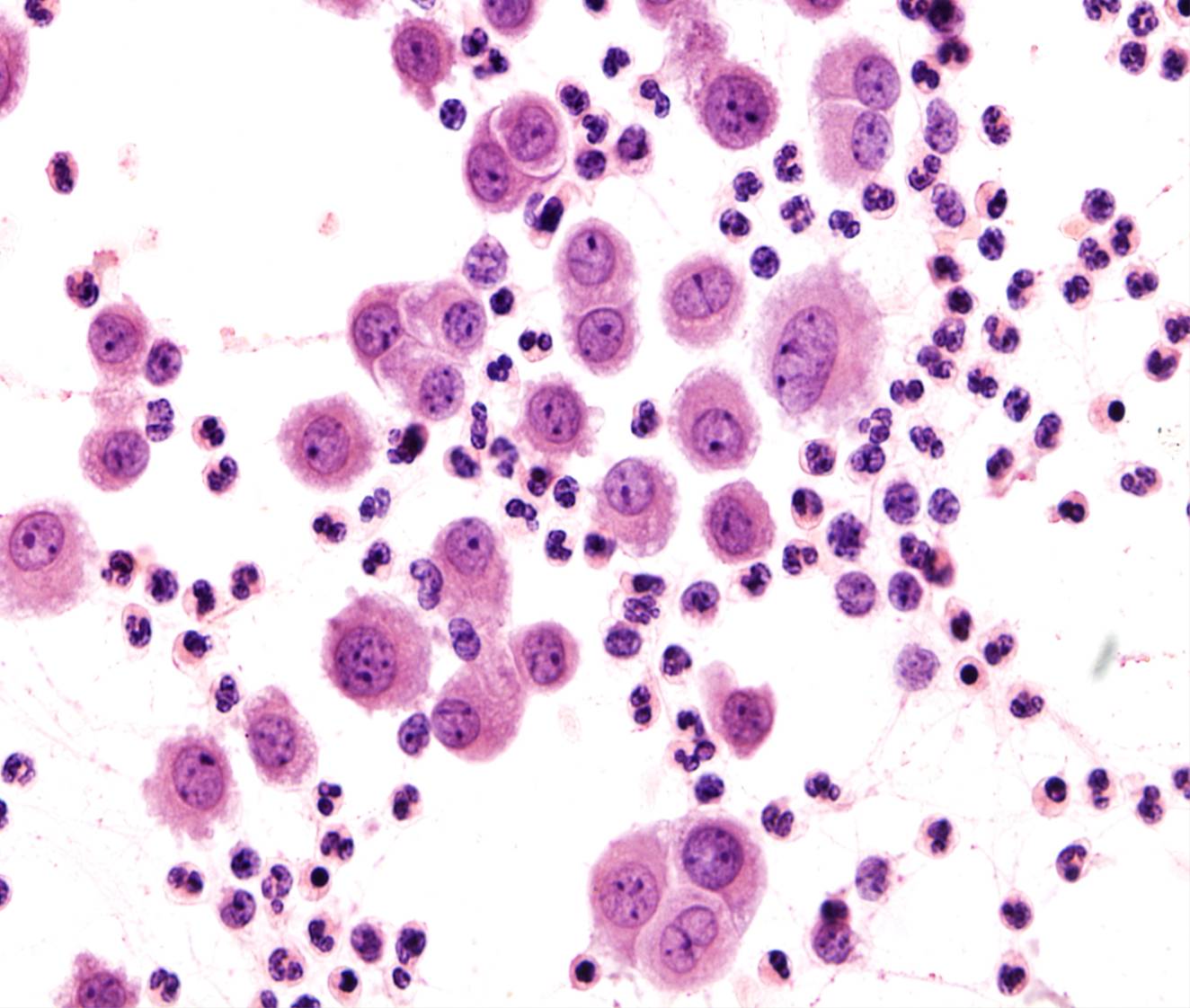
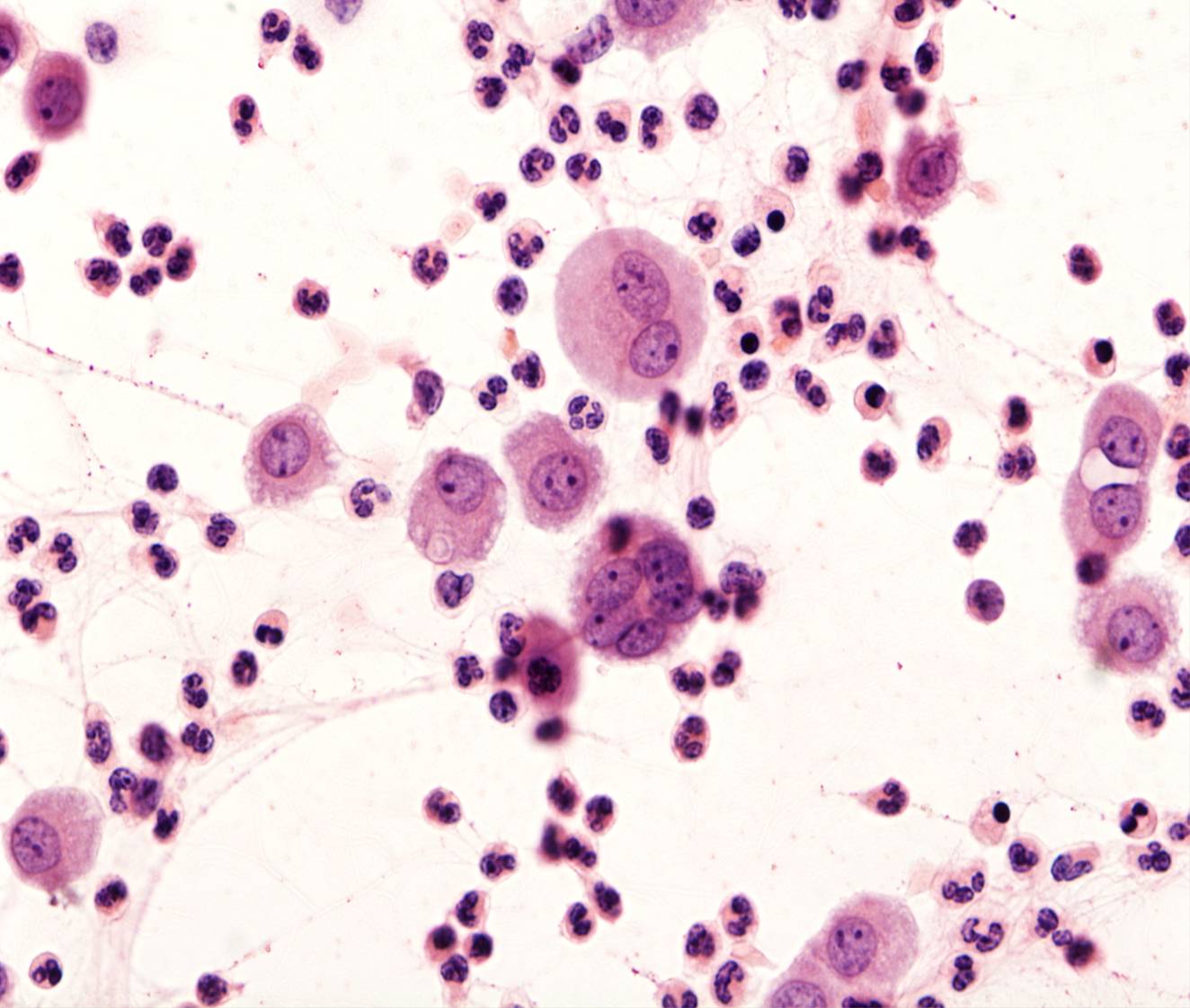
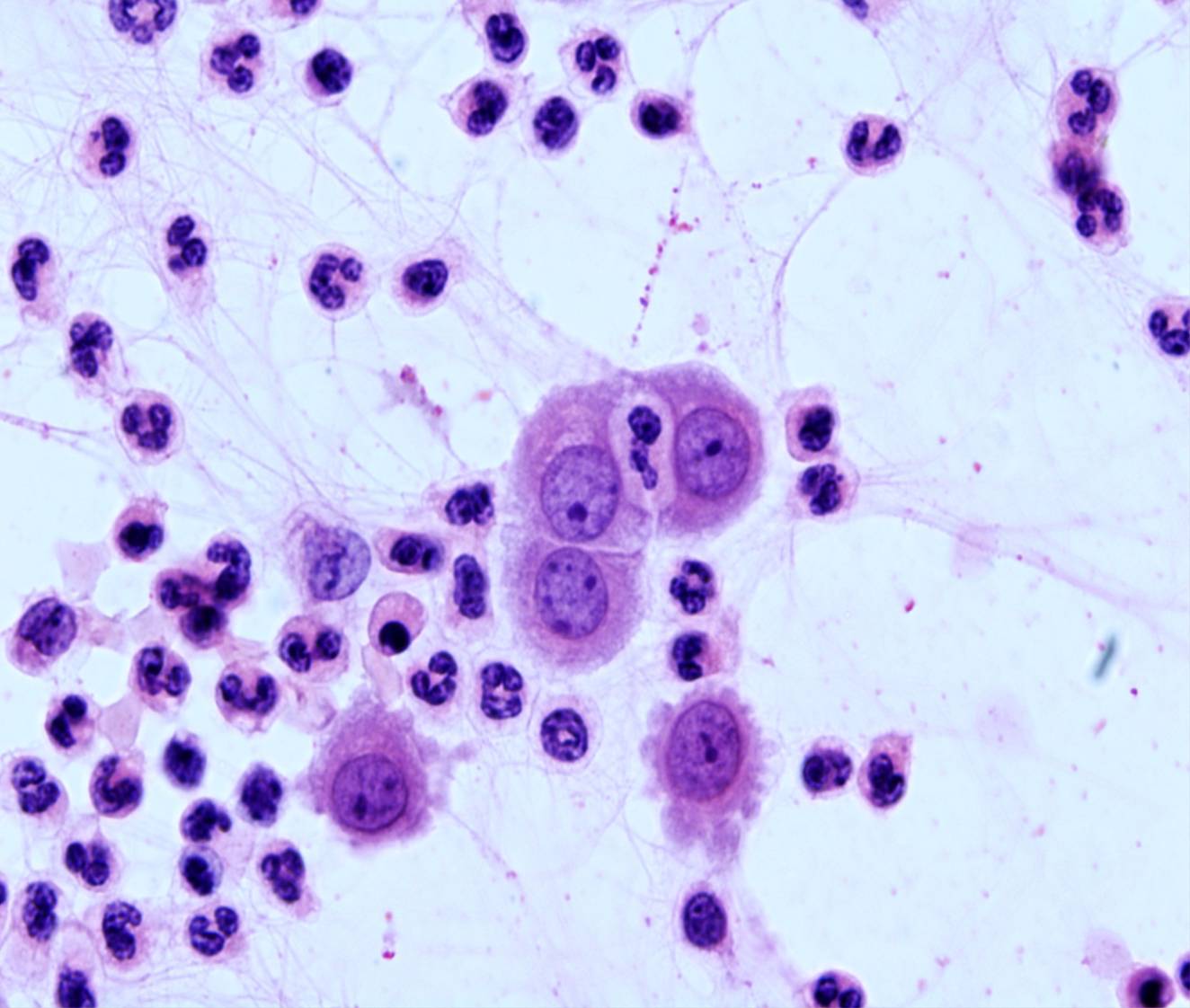
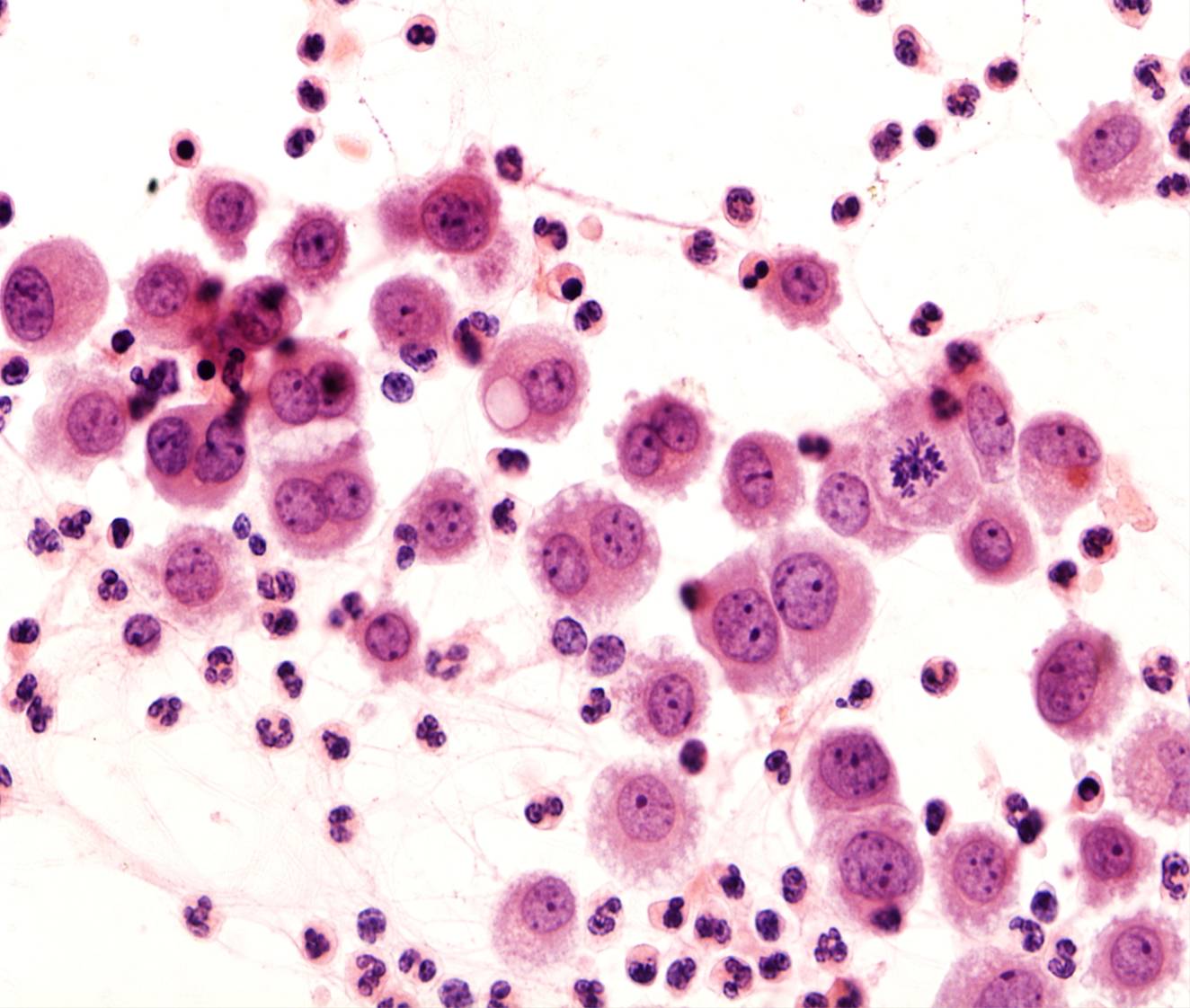
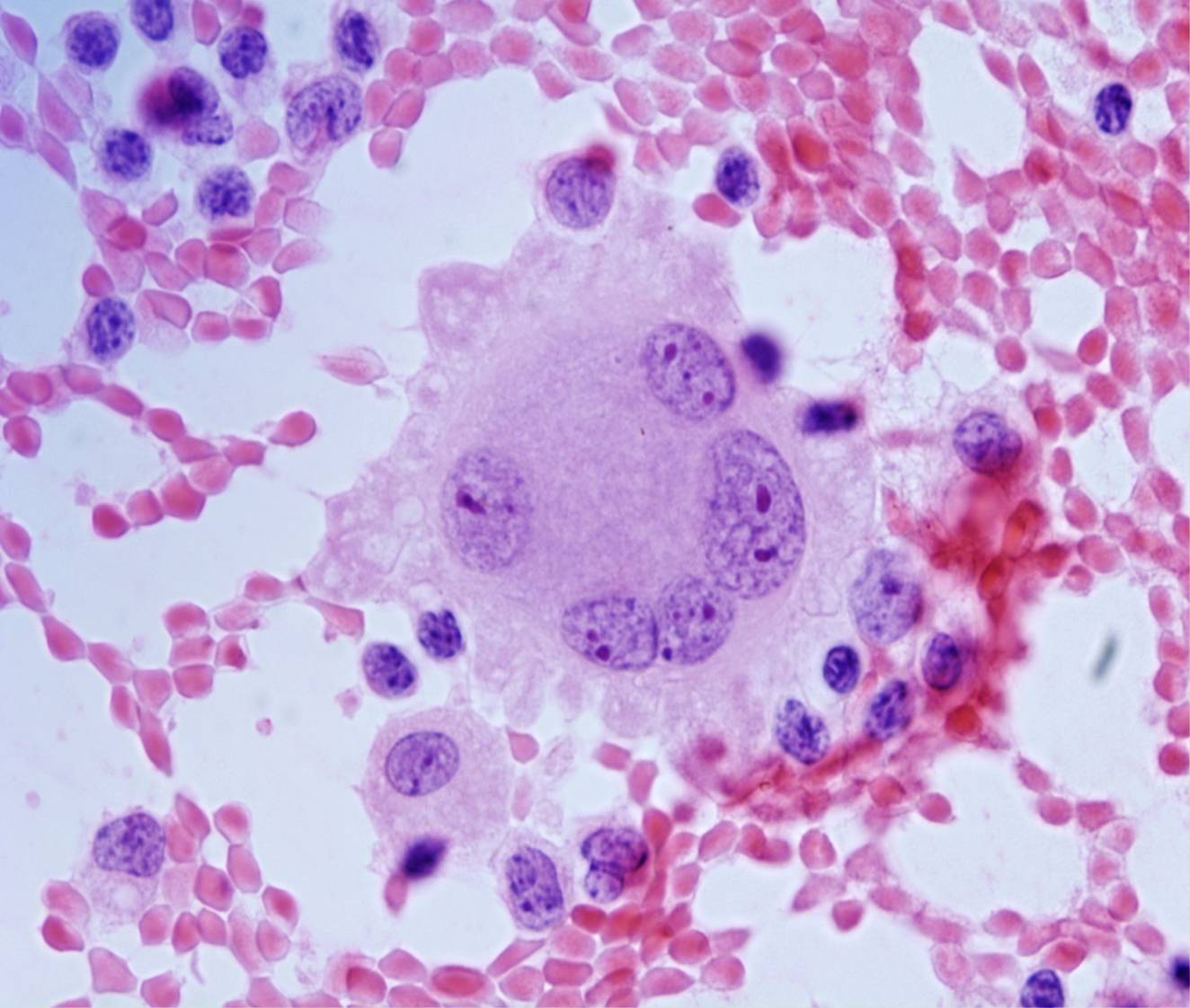
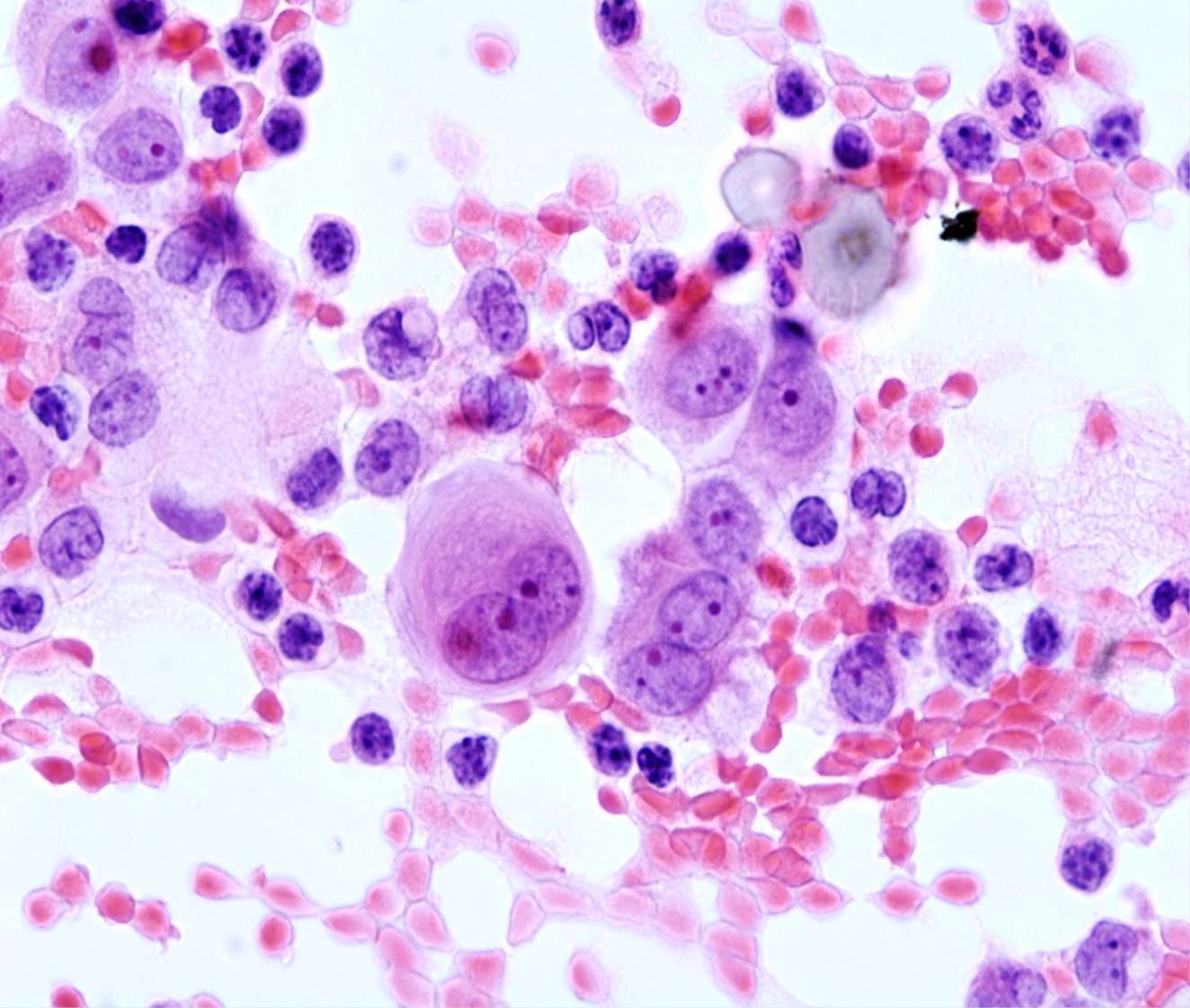
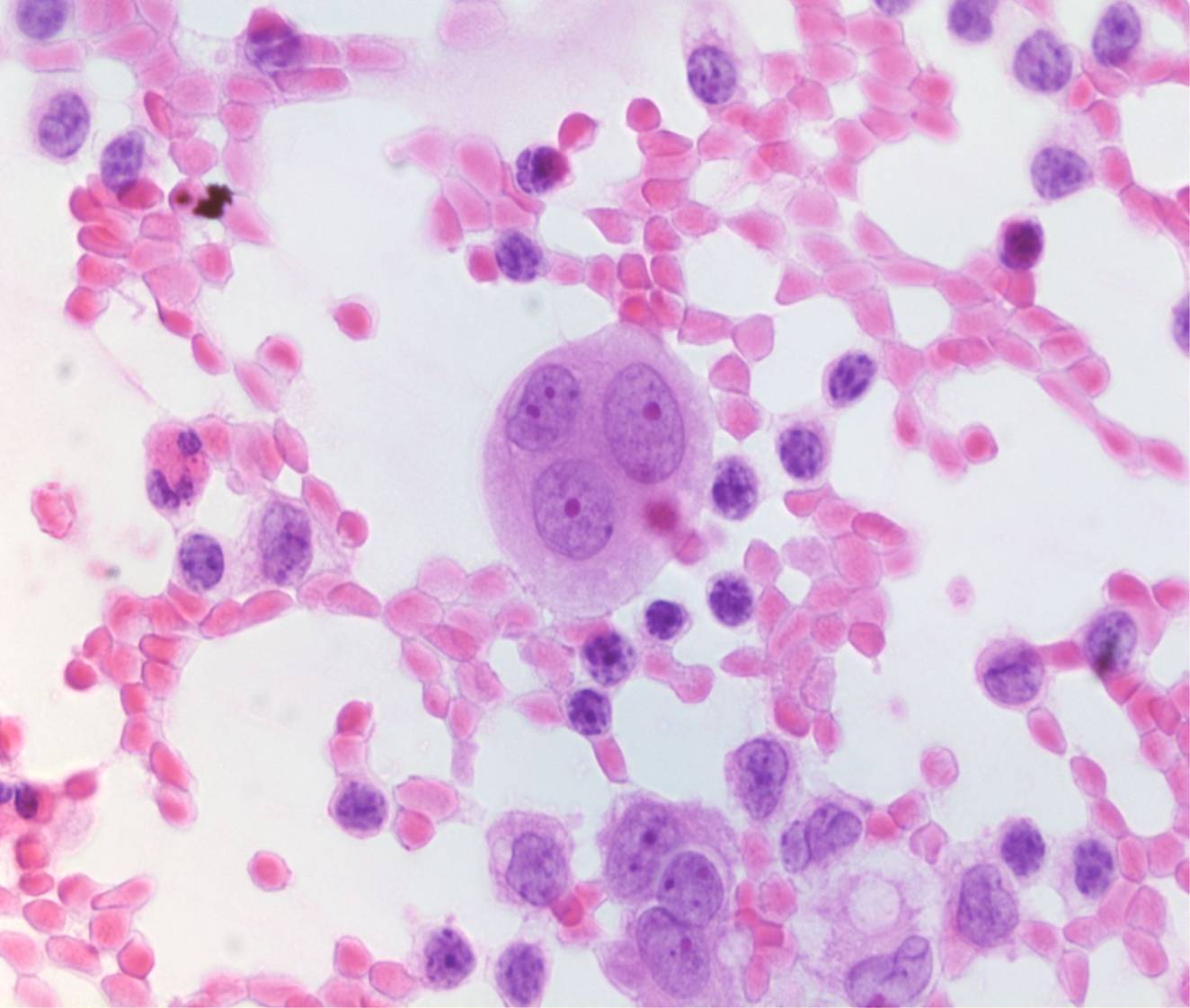
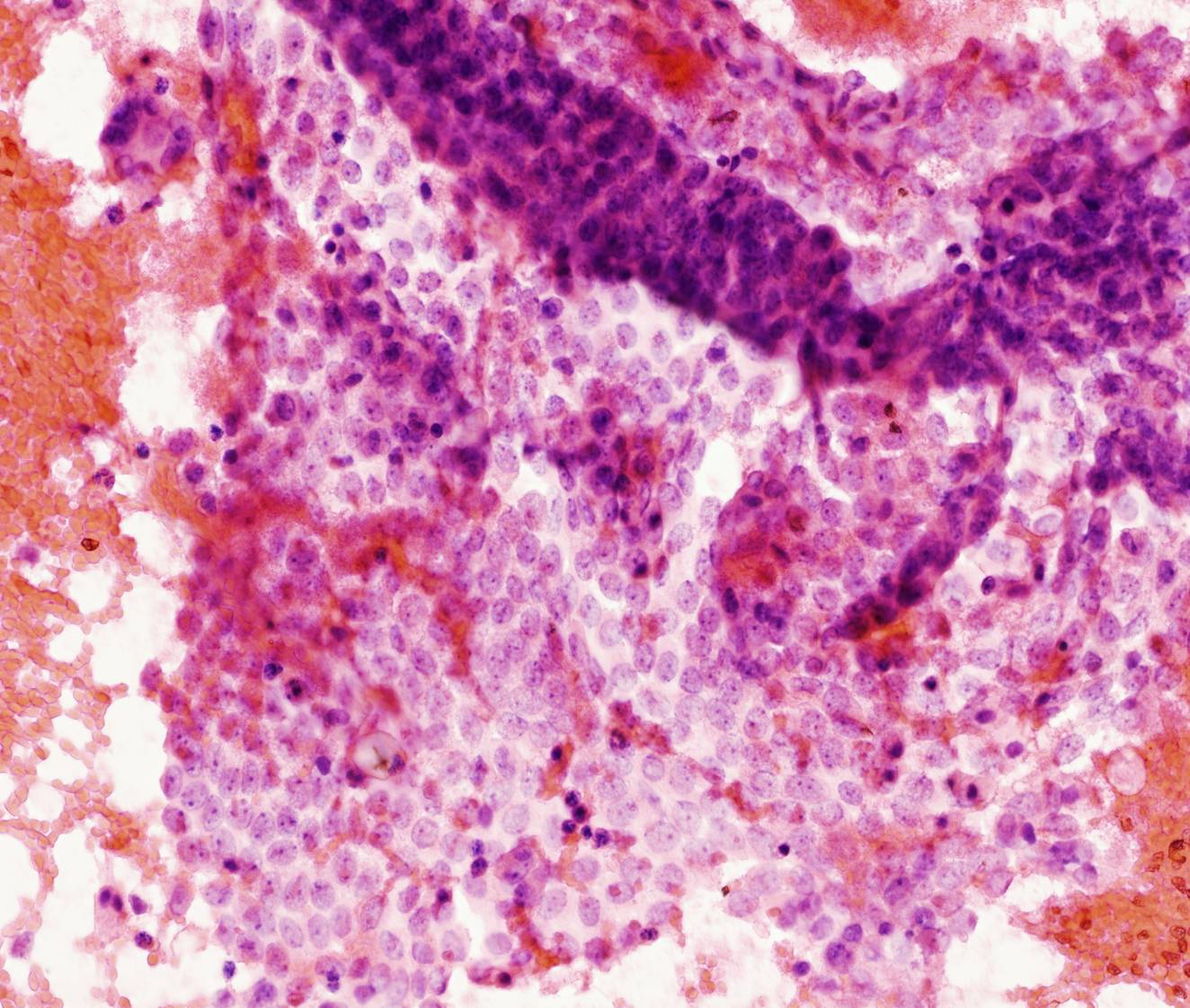
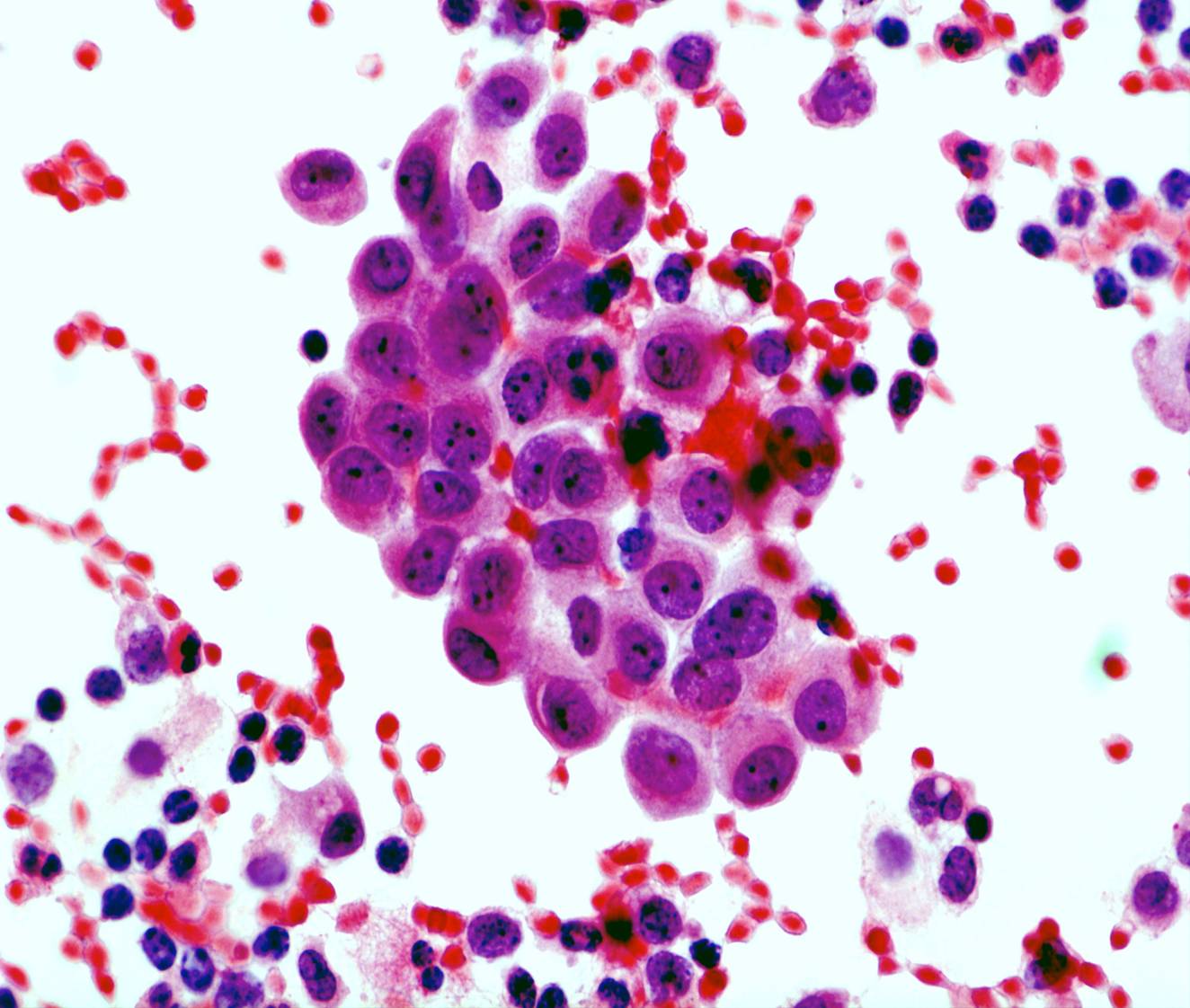
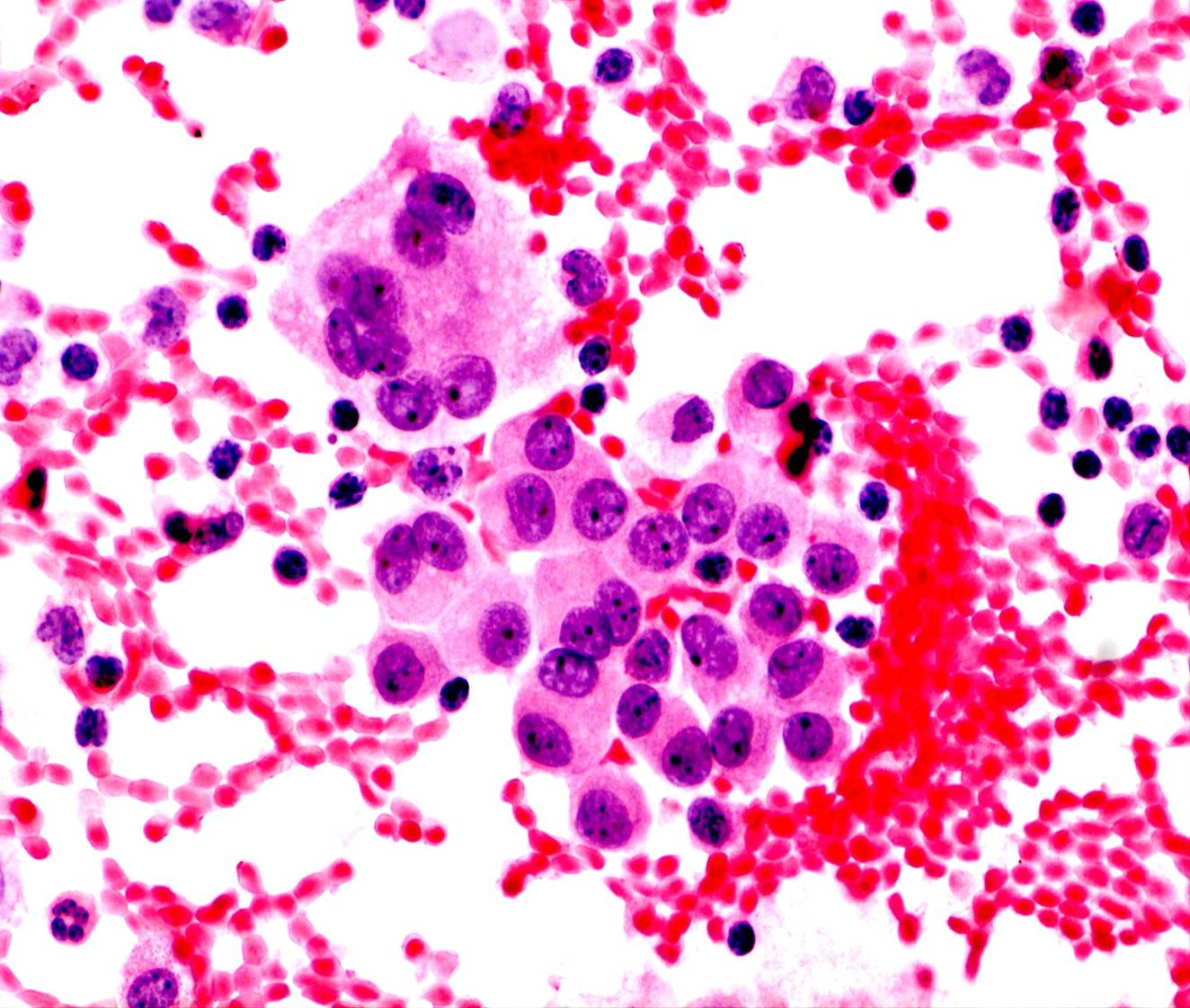
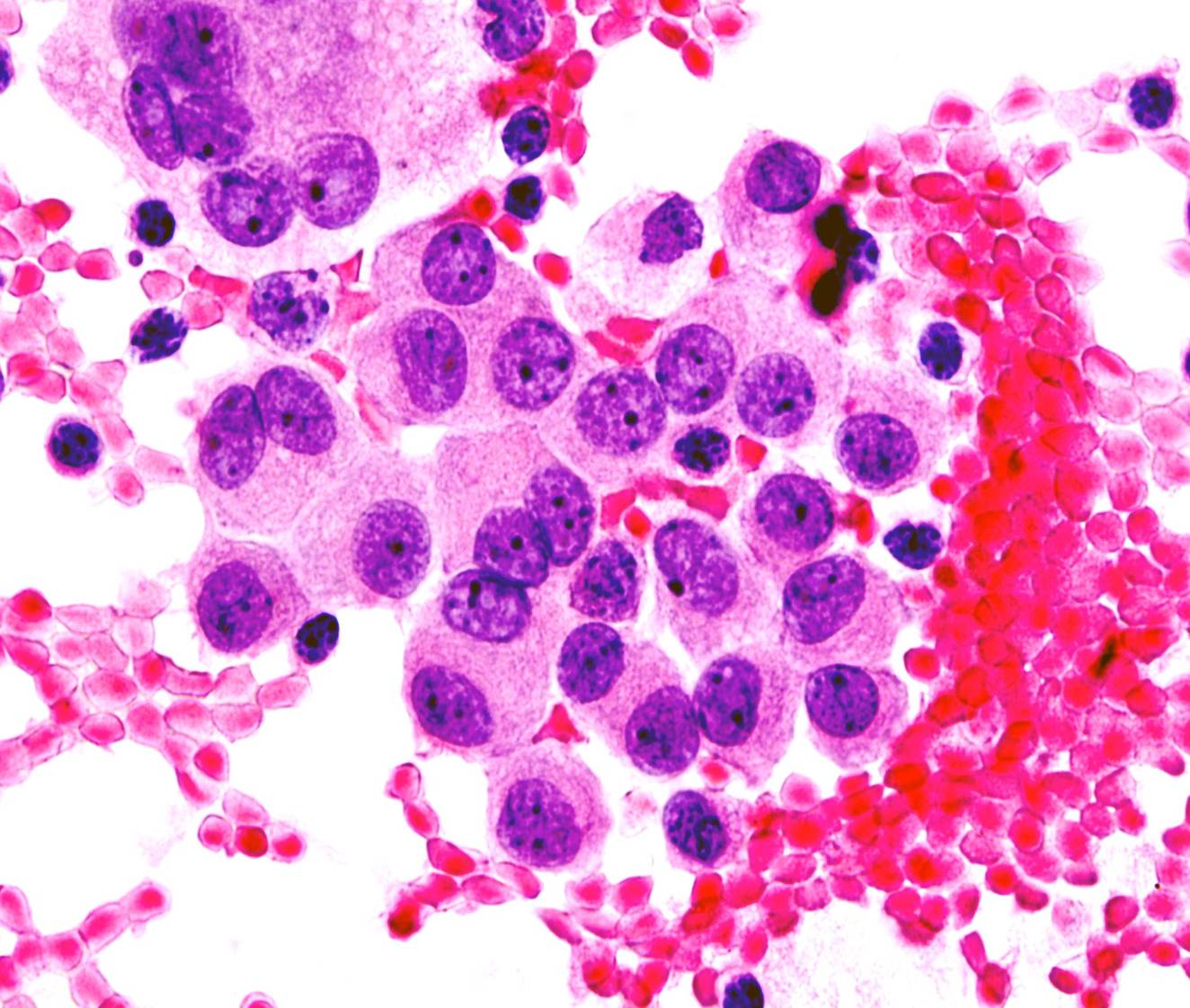
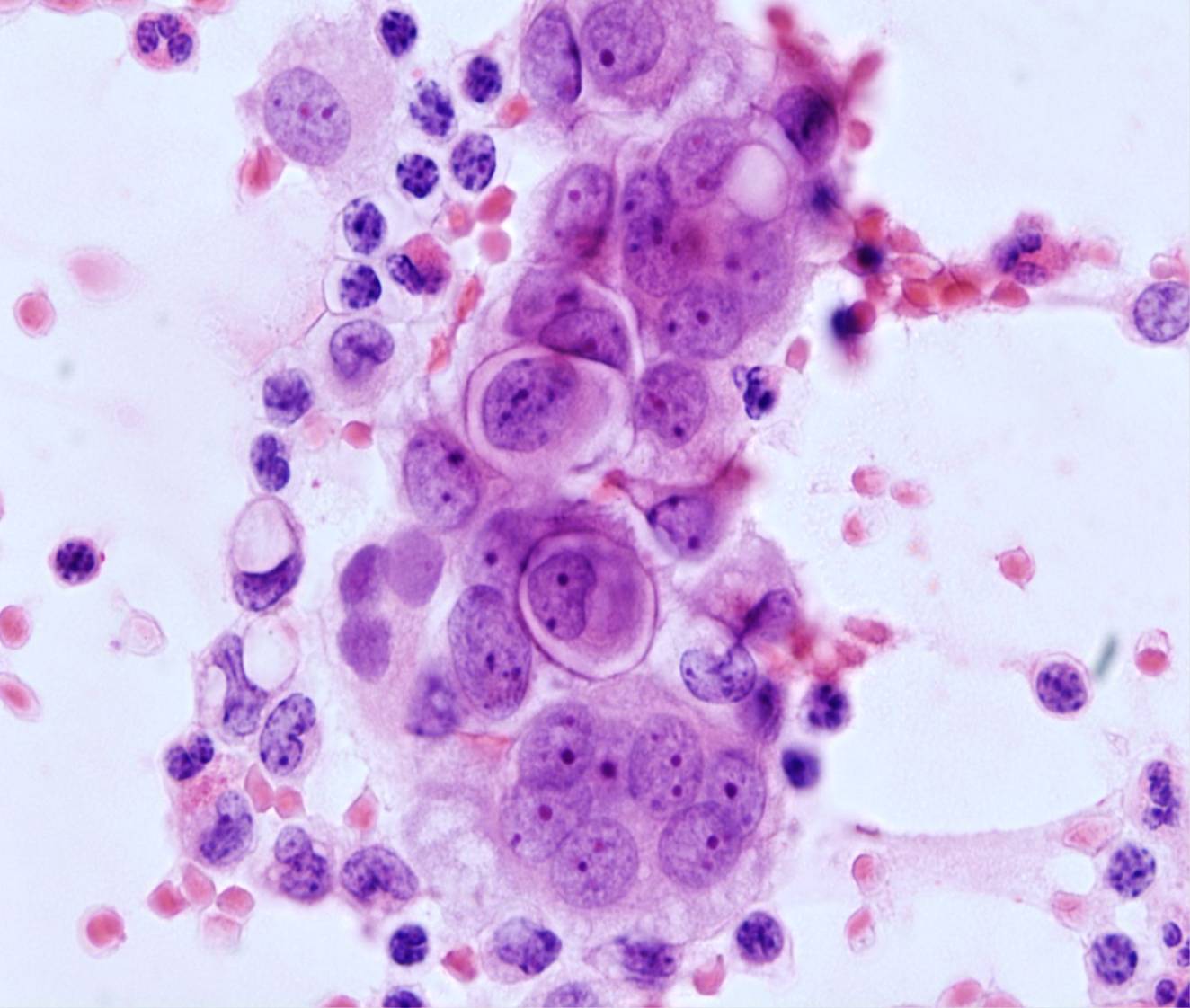
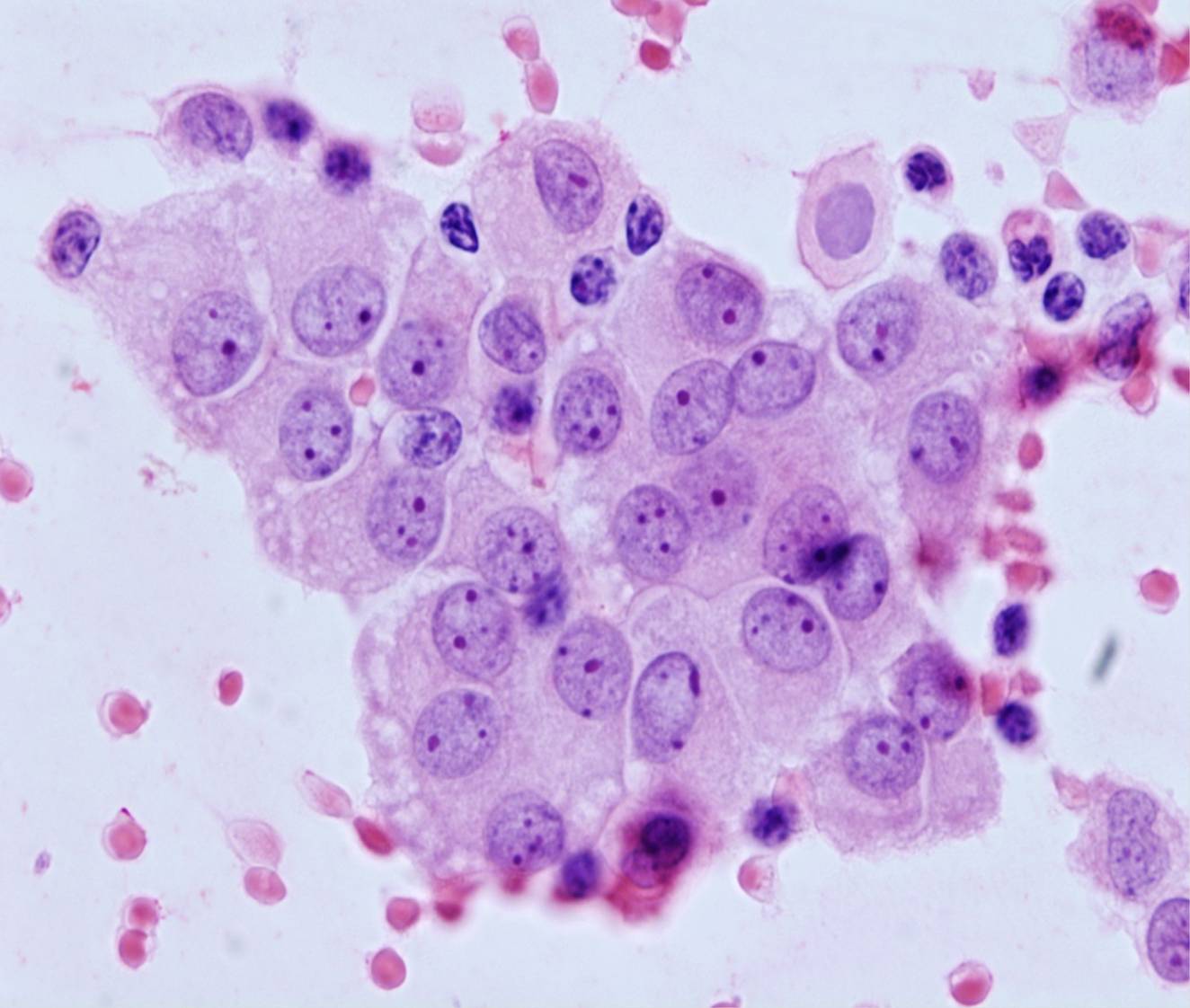
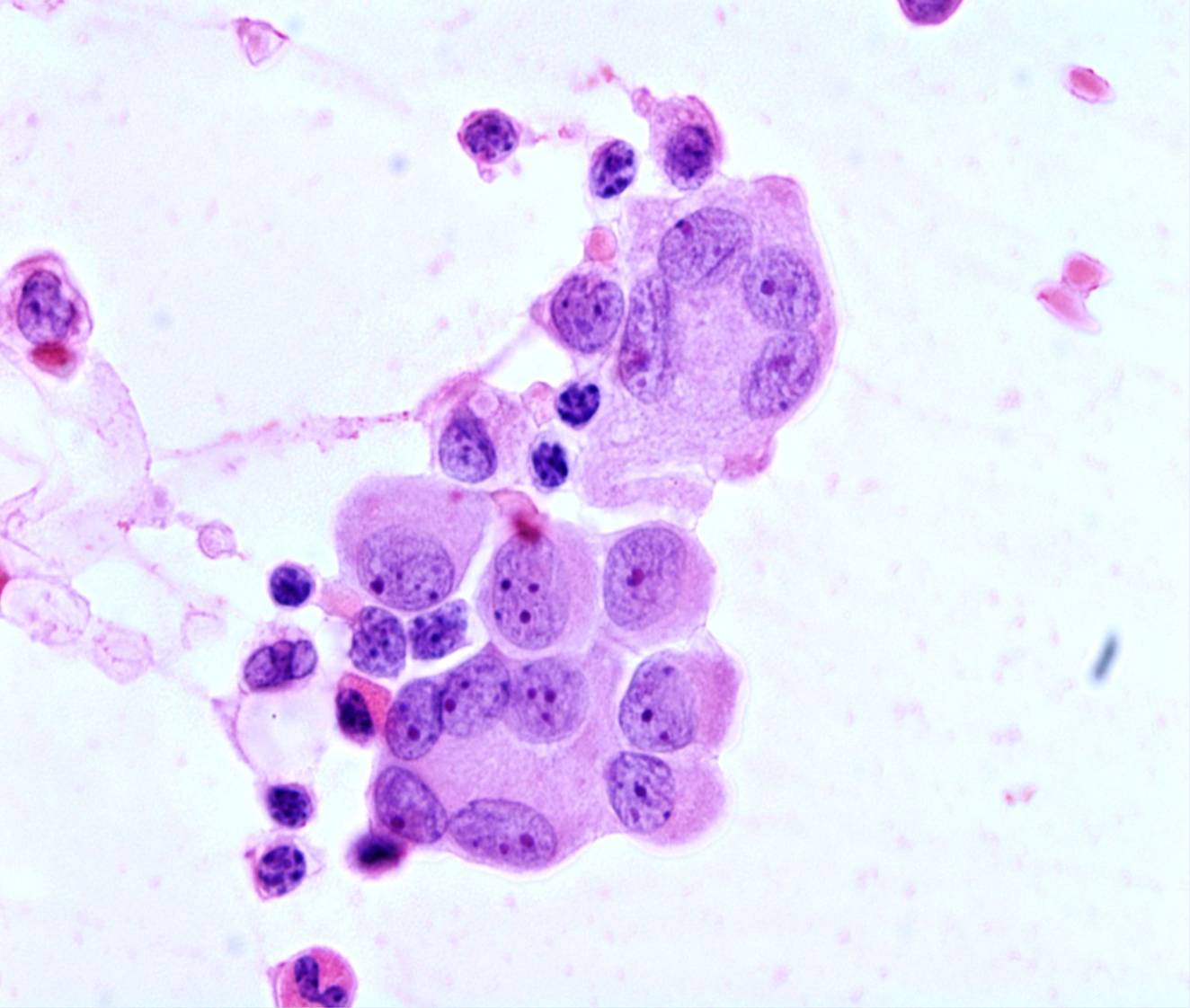
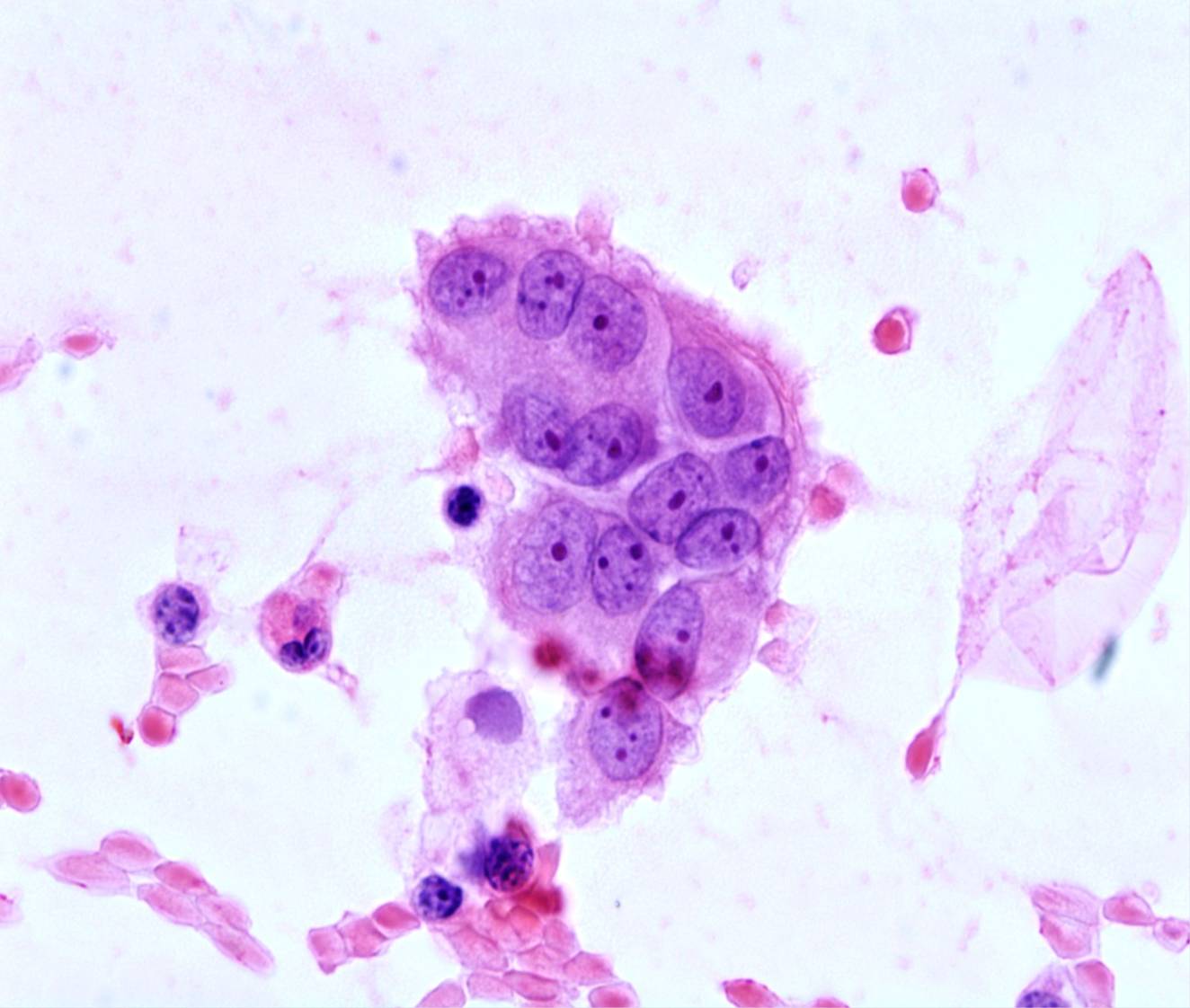
Atypical mesothelial cells
Reactive mesothelial atypia can raise the possibility of a malignancy (primary or metastatic). Reactive mesothelial cells include a spectrum ranging from normal to atypical, the latter showing nuclear pleomorphism, a coarse chromatin texture, irregular nuclear contours, very prominent nucleoli. They are hypertrophic/hyperplastic cells: there is no point in reporting their presence. The clinical history is important: some medical conditions, such as anemia, cirrhosis, lupus, pulmonary infarction or renal failure, are notorious cases of mesothelial atypia.
Causes of mesothelial atypia
- Chronic effusions
- Asbestos
- Chronic renal failure
- Peritoneal dyalisis
- Thromboembolism
- Radiation or chemotherapy
- Cirrhosis
- Pericardial or scrotal effusions
- Acute serositis
- Neoplasms
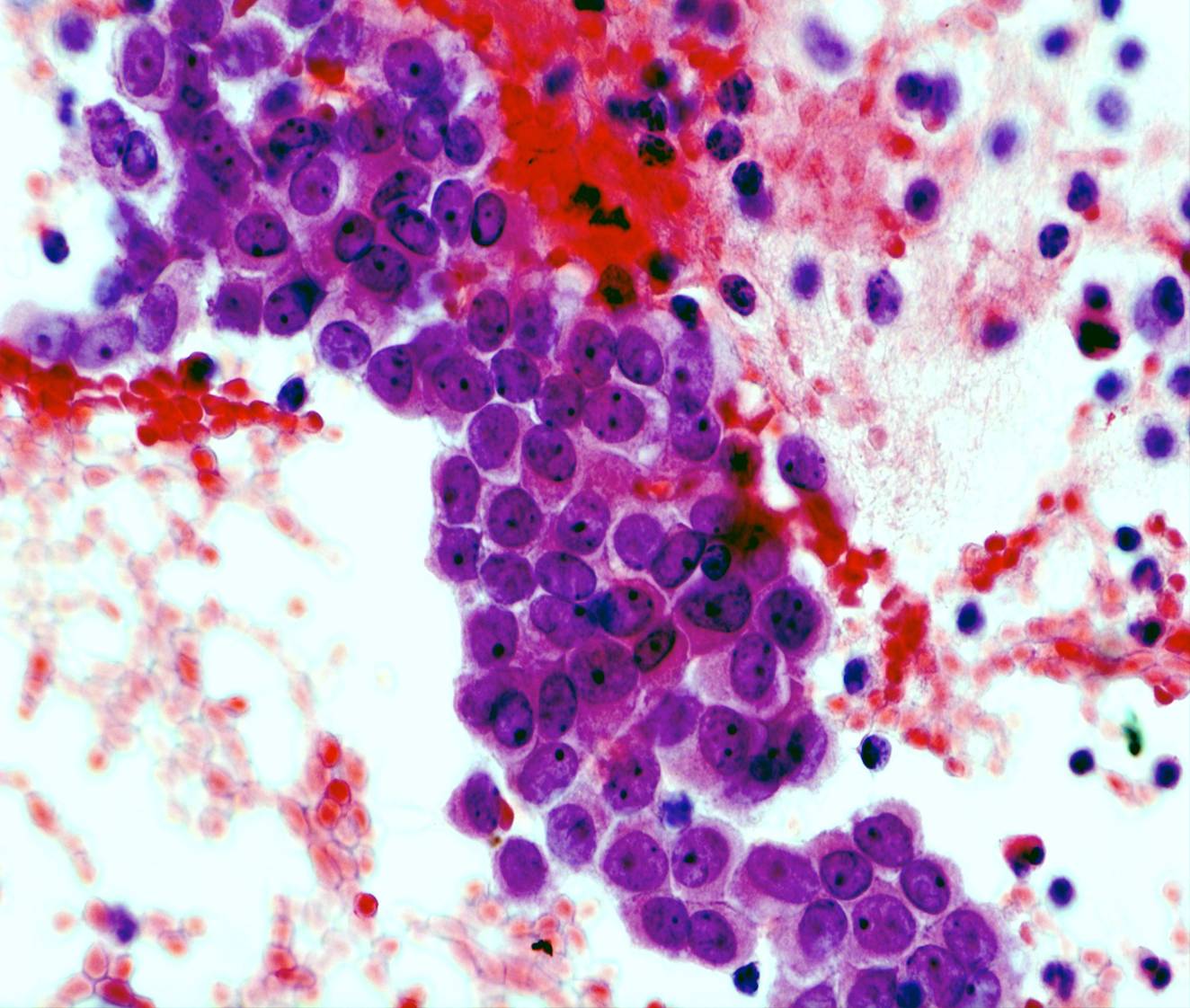
Diagnostic pitfalls
- Papillary fragments of mesothelium
- Giant multinucleated cells
- Overstaining
- Smear of poor quality
Good quality and well stained smears are helpful in avoiding overdiagnosis. Any doubts should be stated in the report.
2 3 4 5 6
8 9 10 11 12
14 15 16 17 18
20 21 22 23 24
26 27 28 29 30
32 33 34
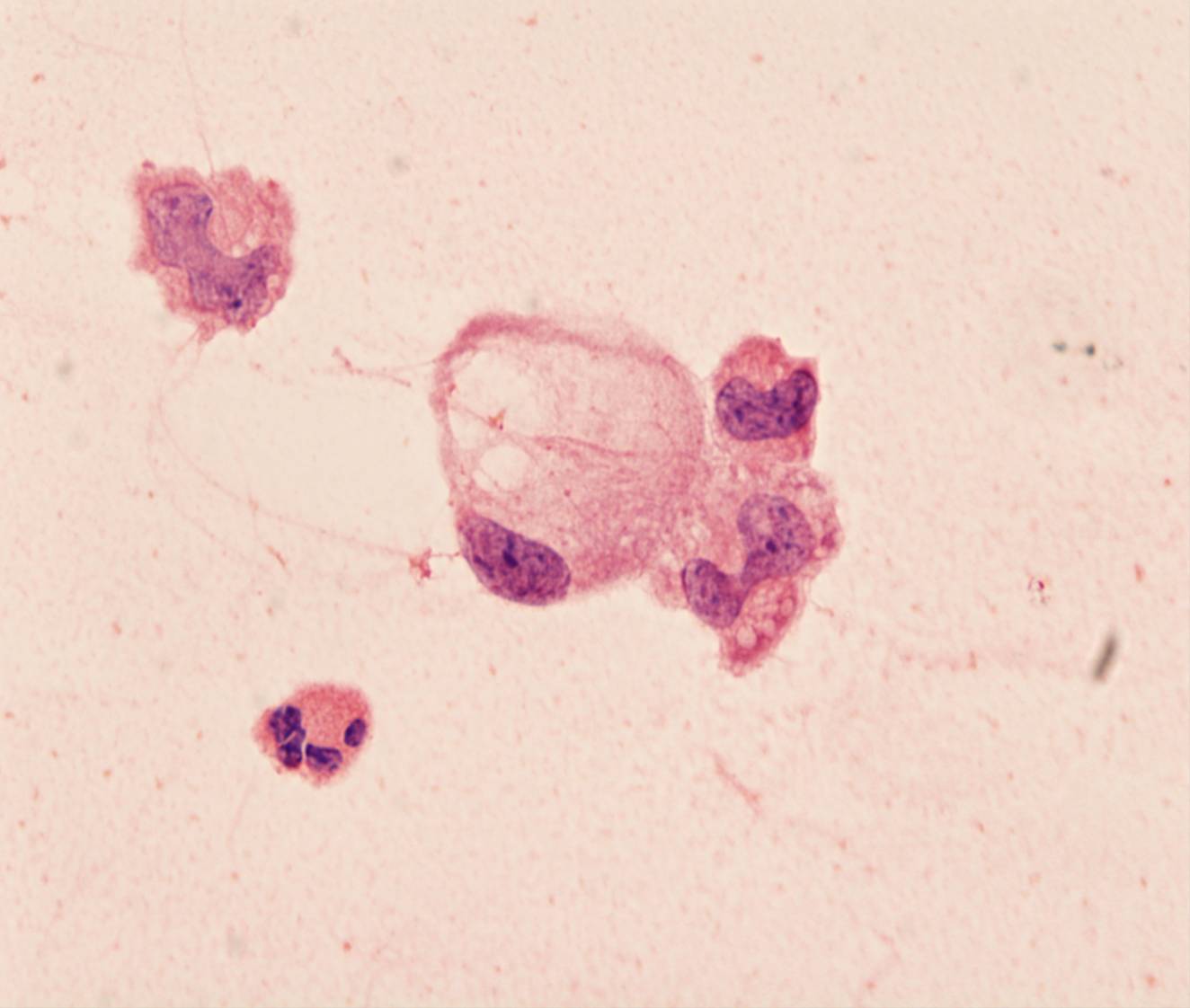
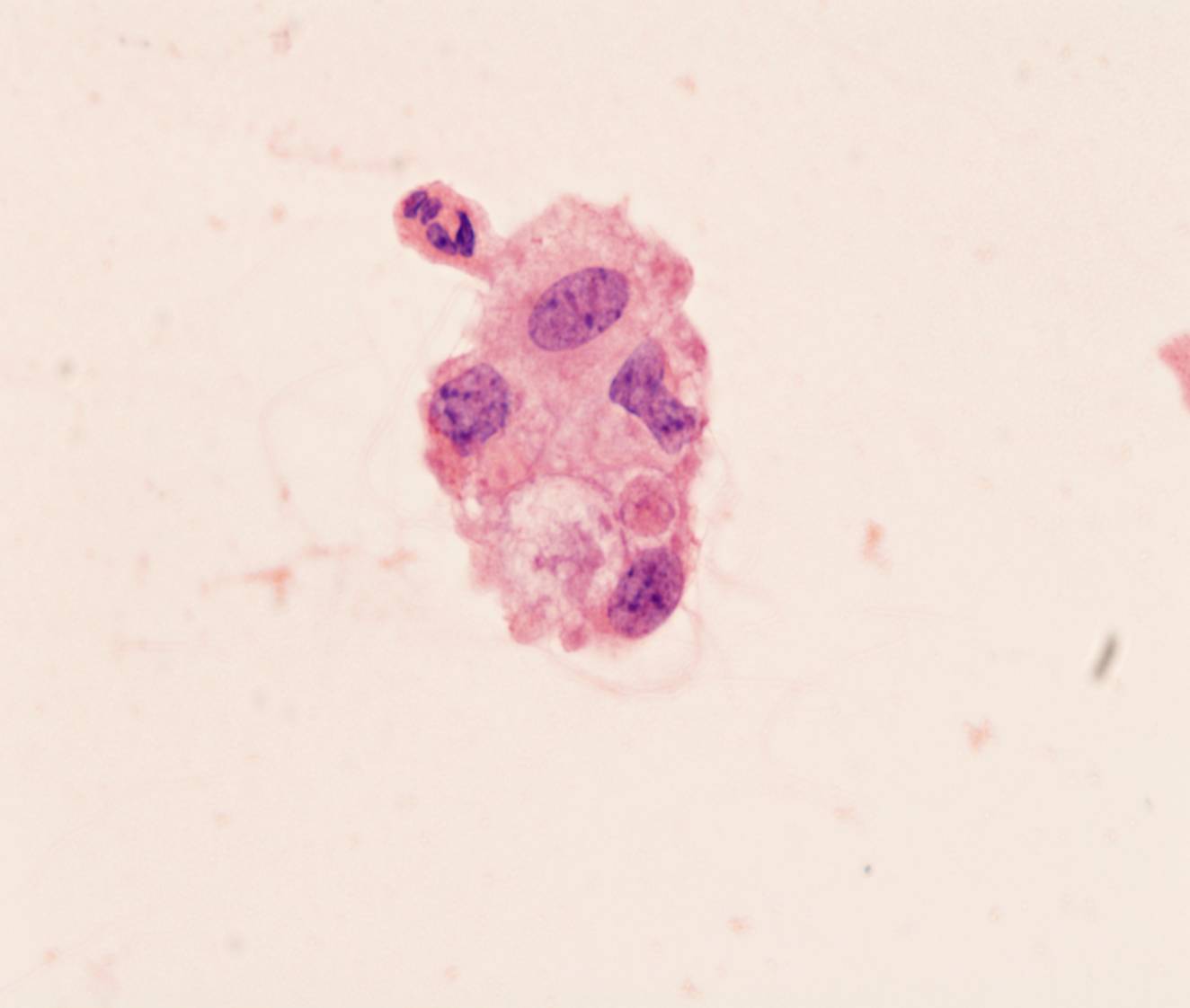
36 37 Macrophages
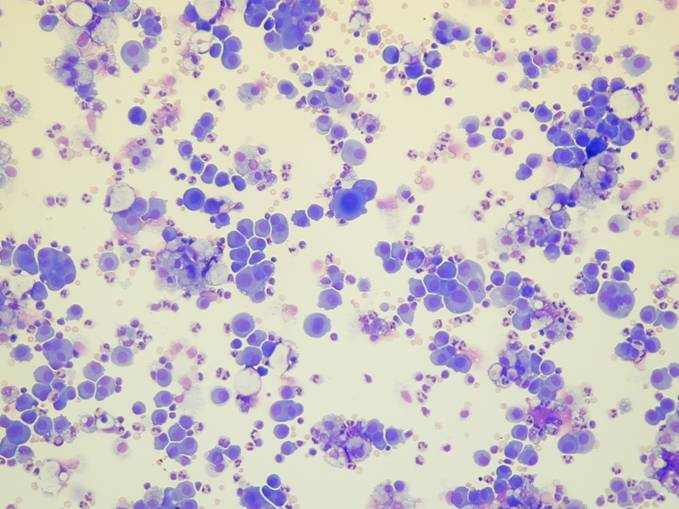
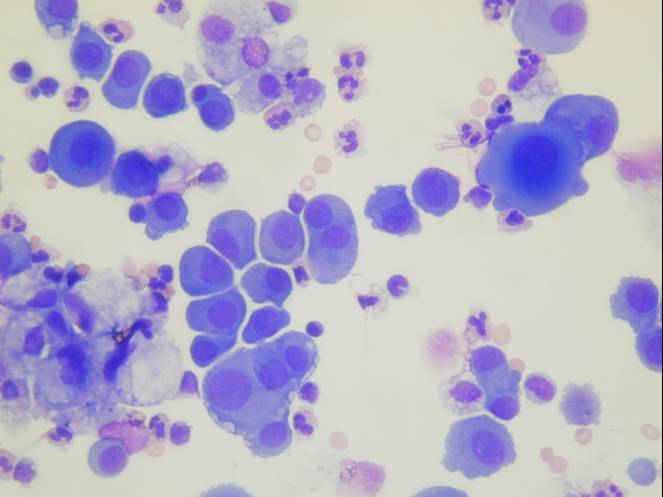
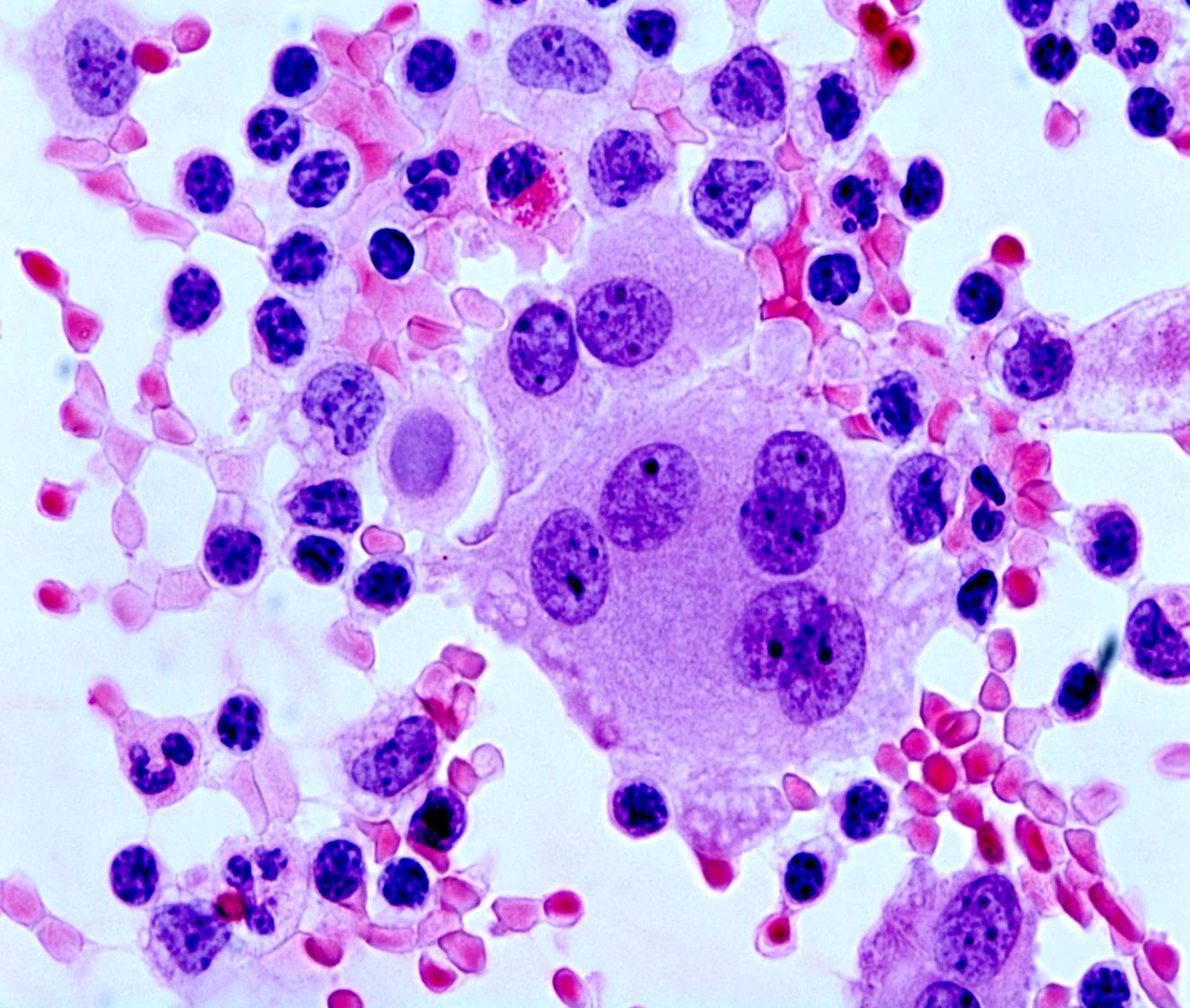
- Smaller nuclei than those of mesothelial cells
- Often folded nuclei
- Binucleation, multinucleation
- Granular or vacuolated cytoplasm
- Phagocytosis
- Sheets and groups
- No 'windows' between adjacent cells
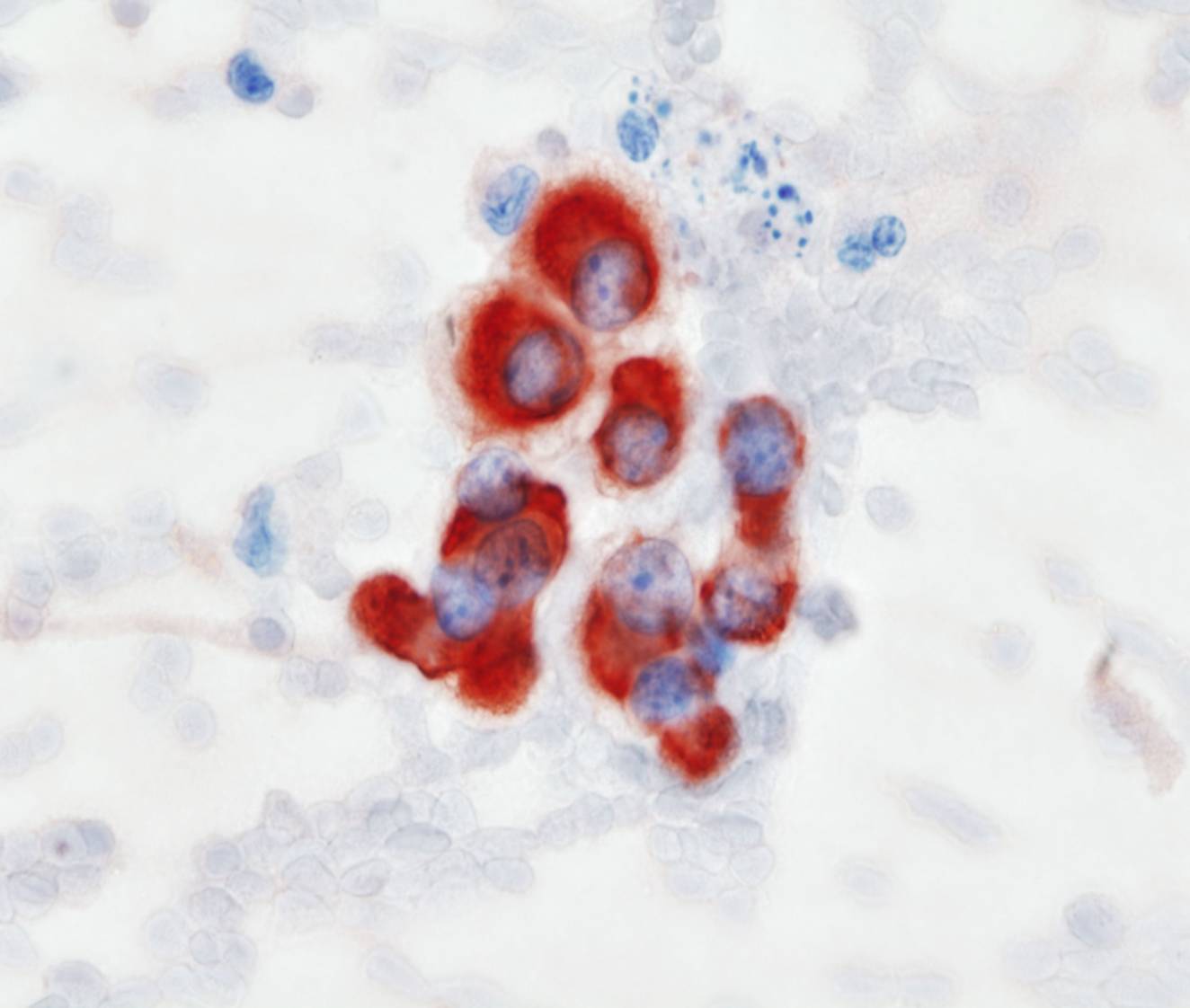
Immunocytochemistry, although rarely if ever necessary, can distinguish histiocytes from mesothelial cells: the former are positive for CD68 and negative for keratin proteins, the reverse is true for the latter.
Some effusions may also contain many lymphocytes.
39 40 41 42 43
45 46 47 48 49