| Anatomy and histology of the pancreas |
| Fine needle aspiration (FNA) and other sampling methods |
| Reporting terminology |
| Normal cells |
| Pancreatitis |
| Pancreatic cysts |
| Solid tumors |
| Biliary tract cytology |
Pancreatic endocrine tumors
They were previously referred to as islet cell tumors, but the term pancreatic endocrine tumors (PET) is more appropriate since they arise from multipotent ductular stem cells in addition to isles of Langerhans. They account for 1-2% of pancreatic tumors. They are located most commonly in the body and the tail and may be solid or cystic (due to central necrosis). Most of them give rise to clinical symptoms related to the hormones they produce (most of the cystic ones are non-functioning).
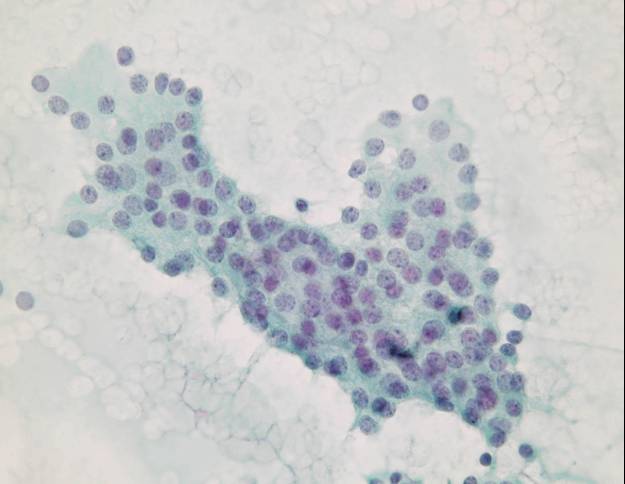
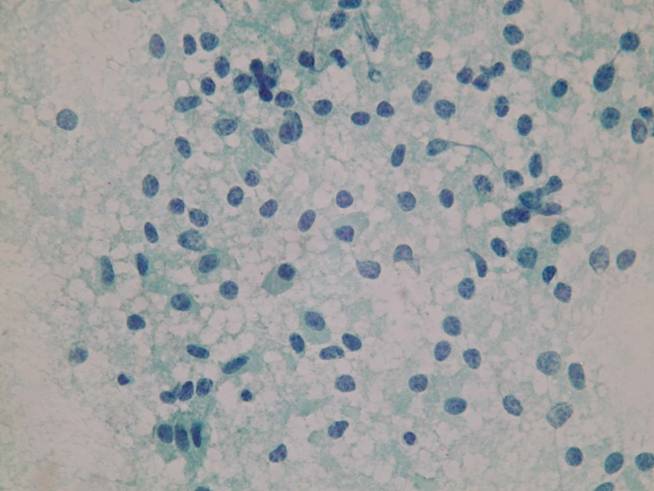
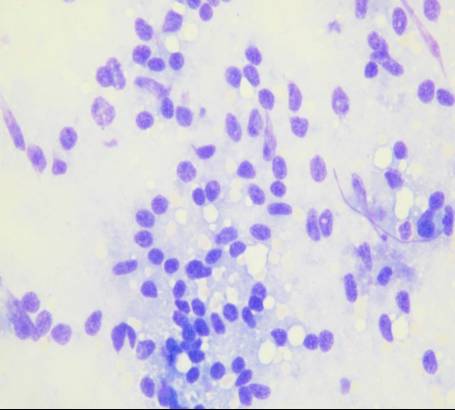
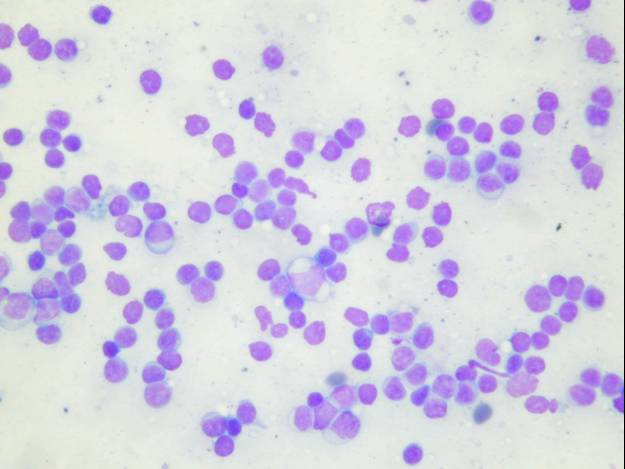
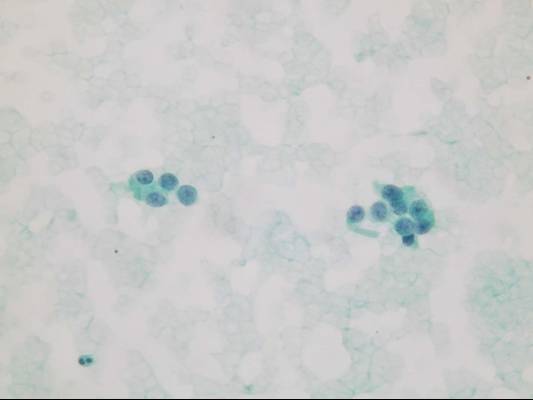
Cytologic diagnostic features
- Highly cellular aspirates with homogeneous small cell population
- Loosely cohesive groups, pseudorosettes, single cells, bare nuclei
- Uniform round to oval nuclei (monotonous appearance)
- Nucleoli not uncommon
- Eccentric nuclei (plasmacytoid appearance)
- Finely stippled (‘salt-and-pepper’) chromatin
- Moderate to abundant cytoplasm
Mitotic figures and rare pleomorphic cells can be present. Cytologic features cannot accurately predict malignant behaviour.
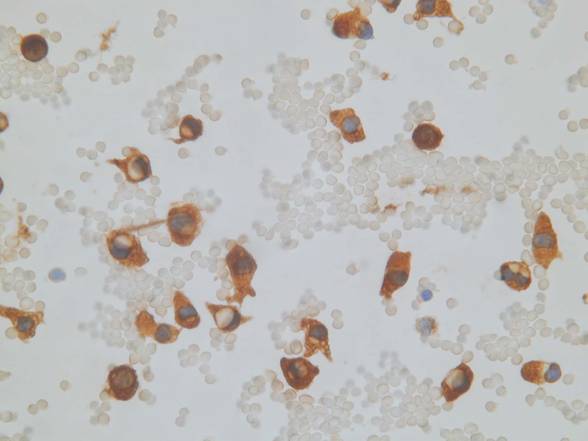
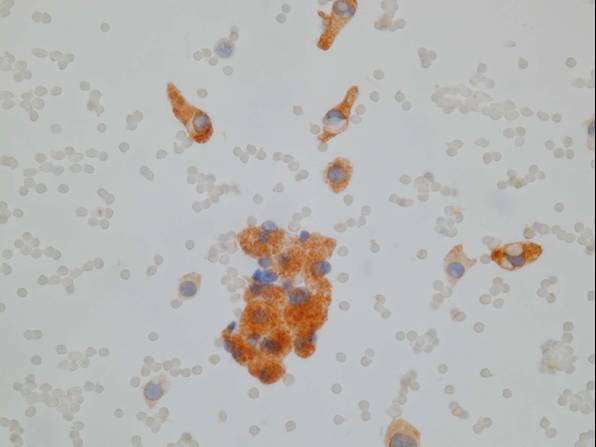
Immunocytochemistry is useful in distinguishing PET from other pancreatic tumors and permits functional characterization of the tumor as well. Tumor cells are positive for chromogranin, synaptophysin, NSE and cytokeratin 8 and 18. They may also express pancreatic peptides or hormones including insulin, glucagon, somatostatin, vasoactive intestinal peptide or gastrin, and ectopic hormones as well (such as ACTH, vasopressin or PTH). Ultrastructural examination reveals dense-core neurosecretory granules.
Differential diagnosis
- Acinar cell carcinoma
- Solid-pseudopapillary tumor
- Undifferentiated neuroendocrine (small cell) carcinoma (primay or metastatic)
- Non-Hodgkin lymphoma
- Metastatic melanoma
- Islet cell hyperplasia
PET lack the necrosis, the mitotic activity and the nuclear molding of undifferentiated neuroendocrine carcinoma. Islet cell hyperplasia may be sampled by FNA in the setting of diabetes, chronic pancreatitis or pancreatic fibrosis secondary to duct obstruction.
Calcitonin