| Physiopathology of the effusions |
| Specimen collection and preparation methods |
| Accuracy |
| Reporting terminology |
| Benign elements |
| Non-neoplastic conditions |
| Malignant effusions |
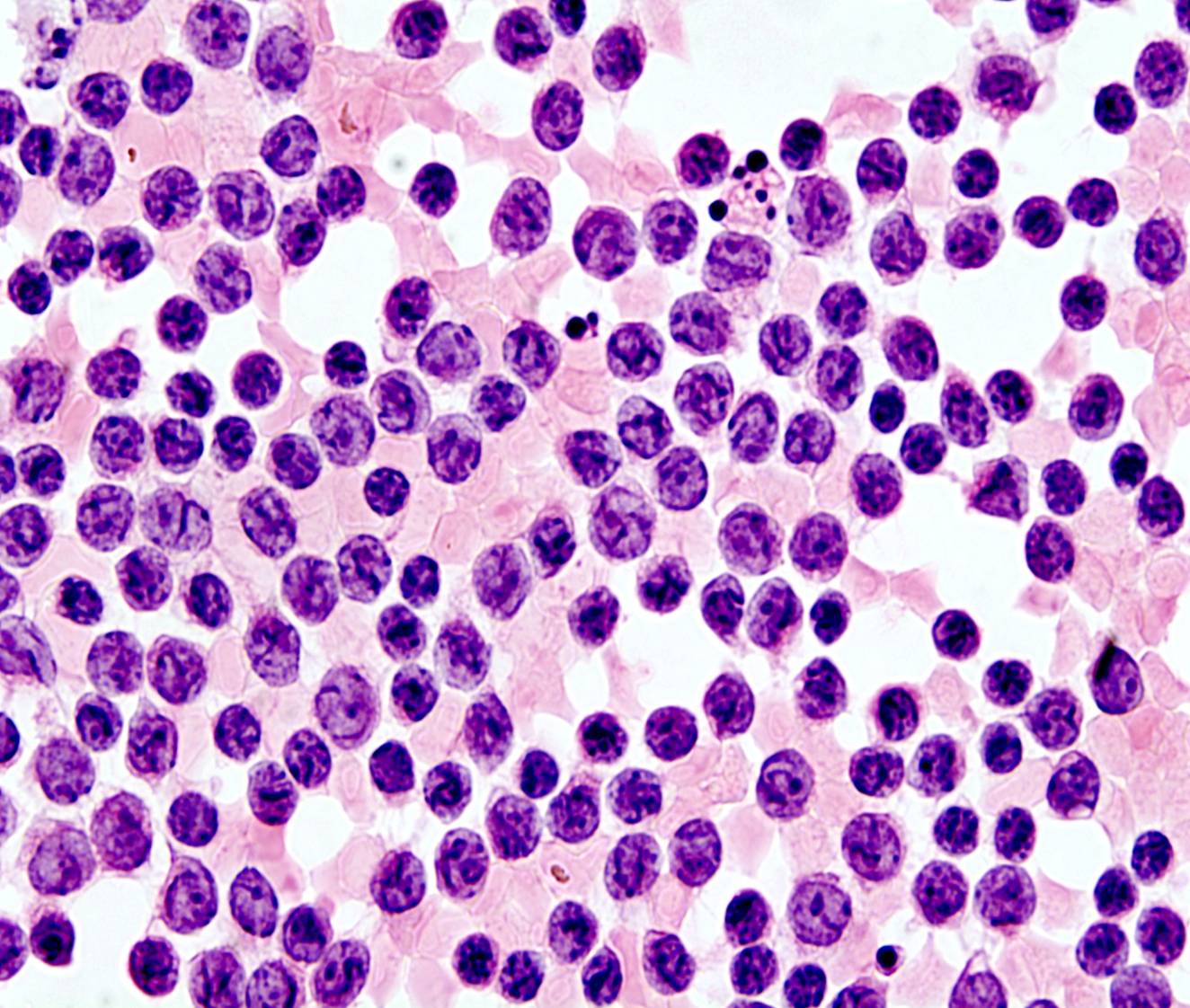
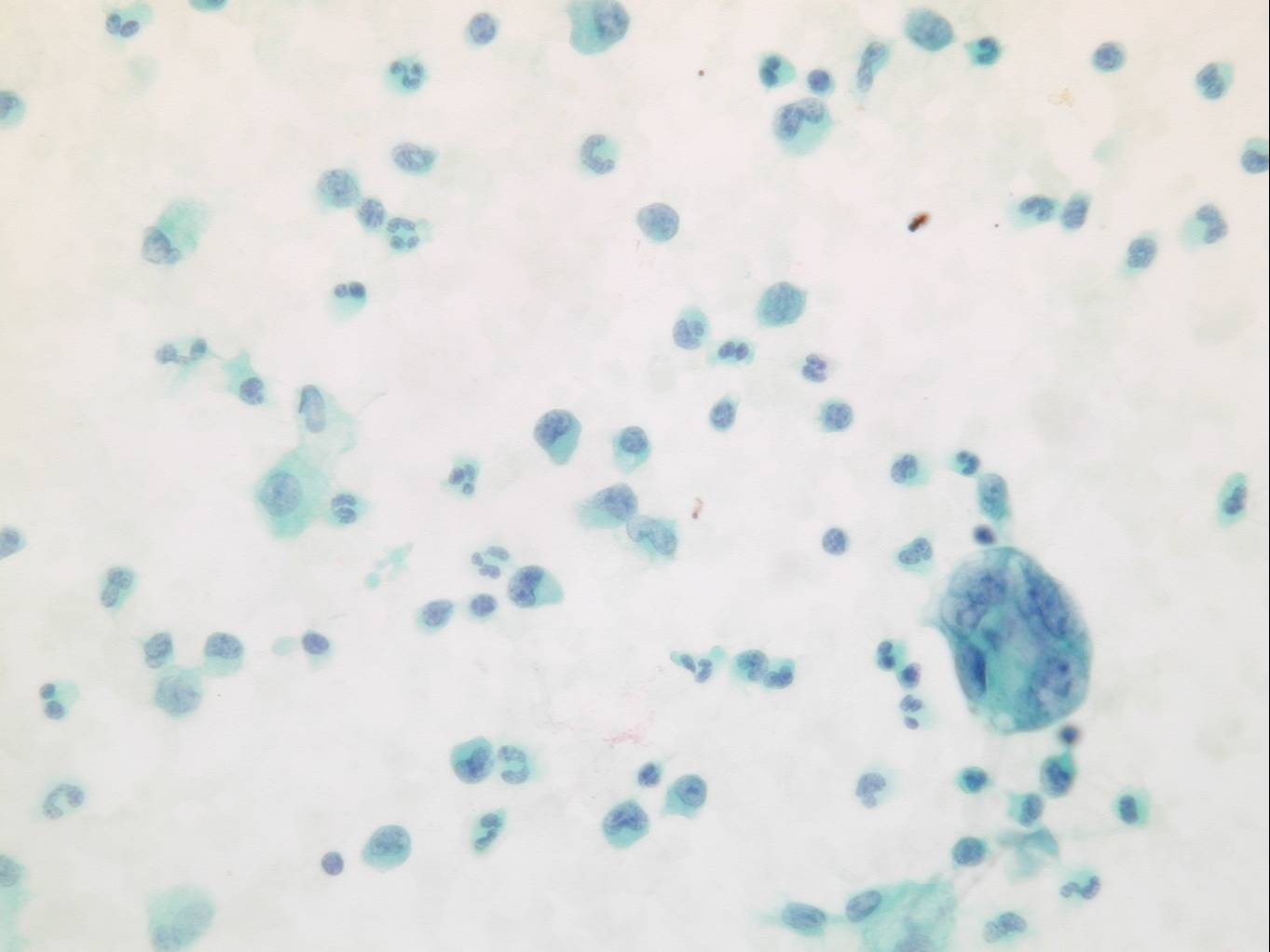
Non-Hodgkin lymphoma
- Monotonous picture
- Dispersed tumor cells
- Few mesothelial cells and macrophages
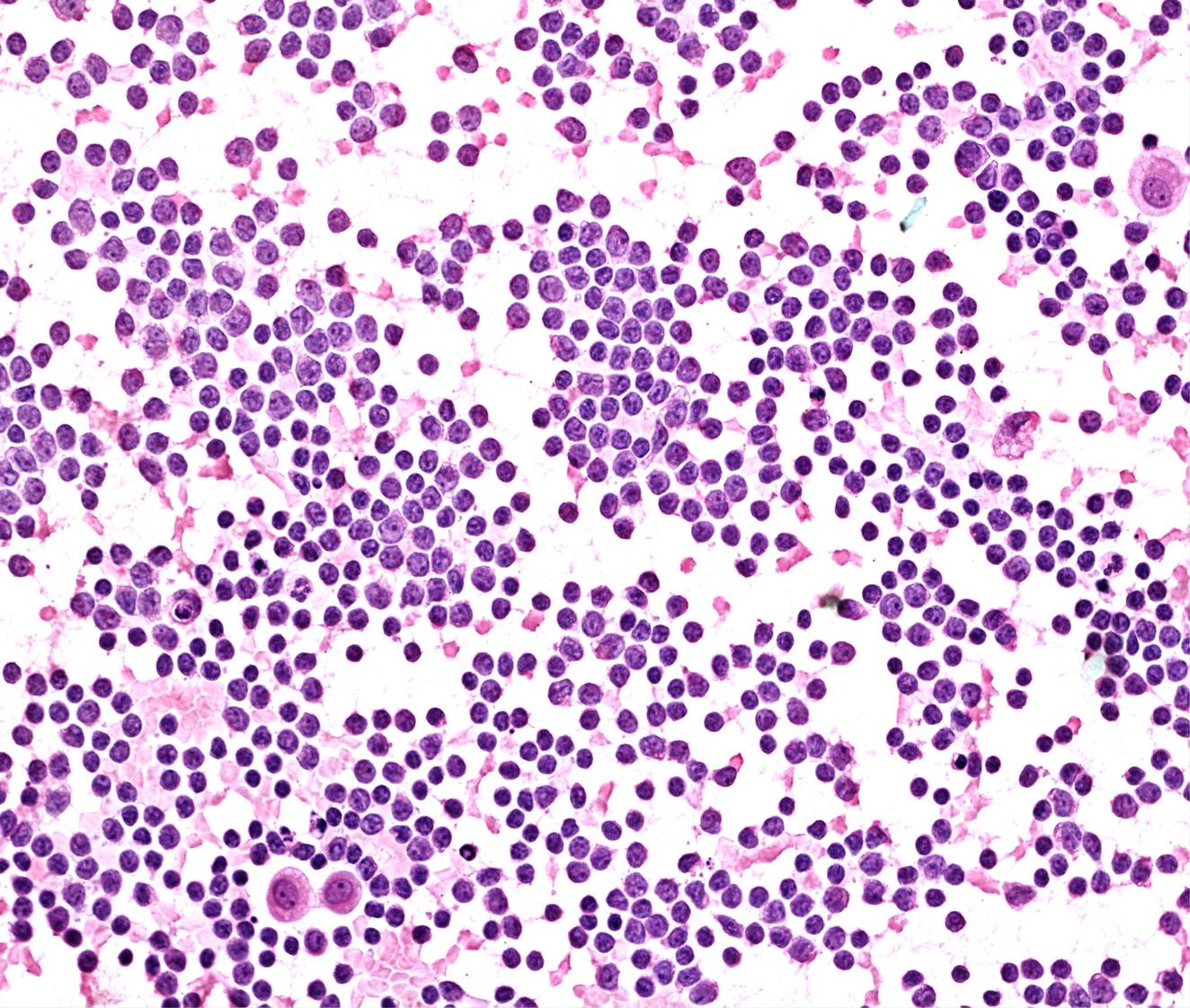
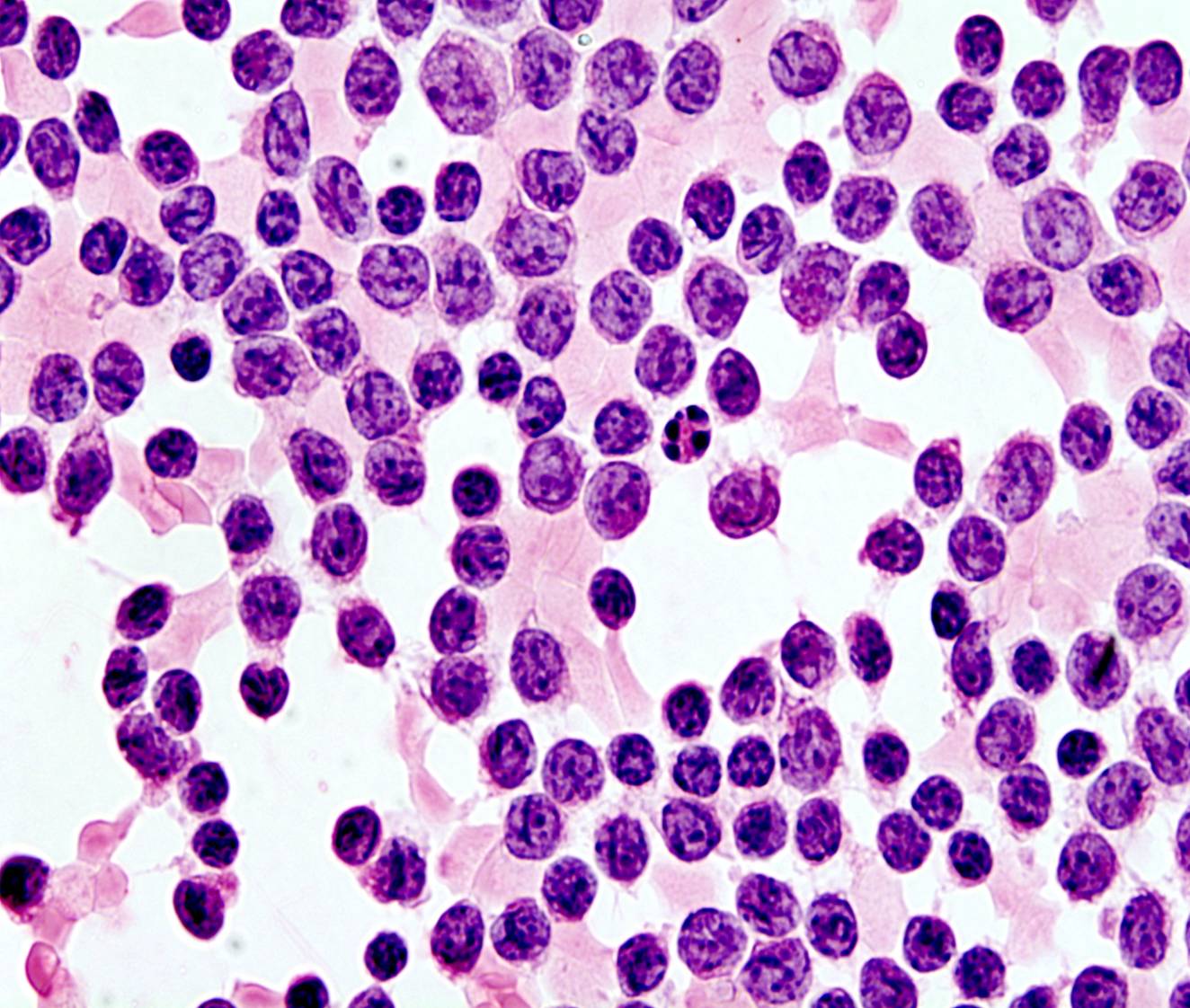
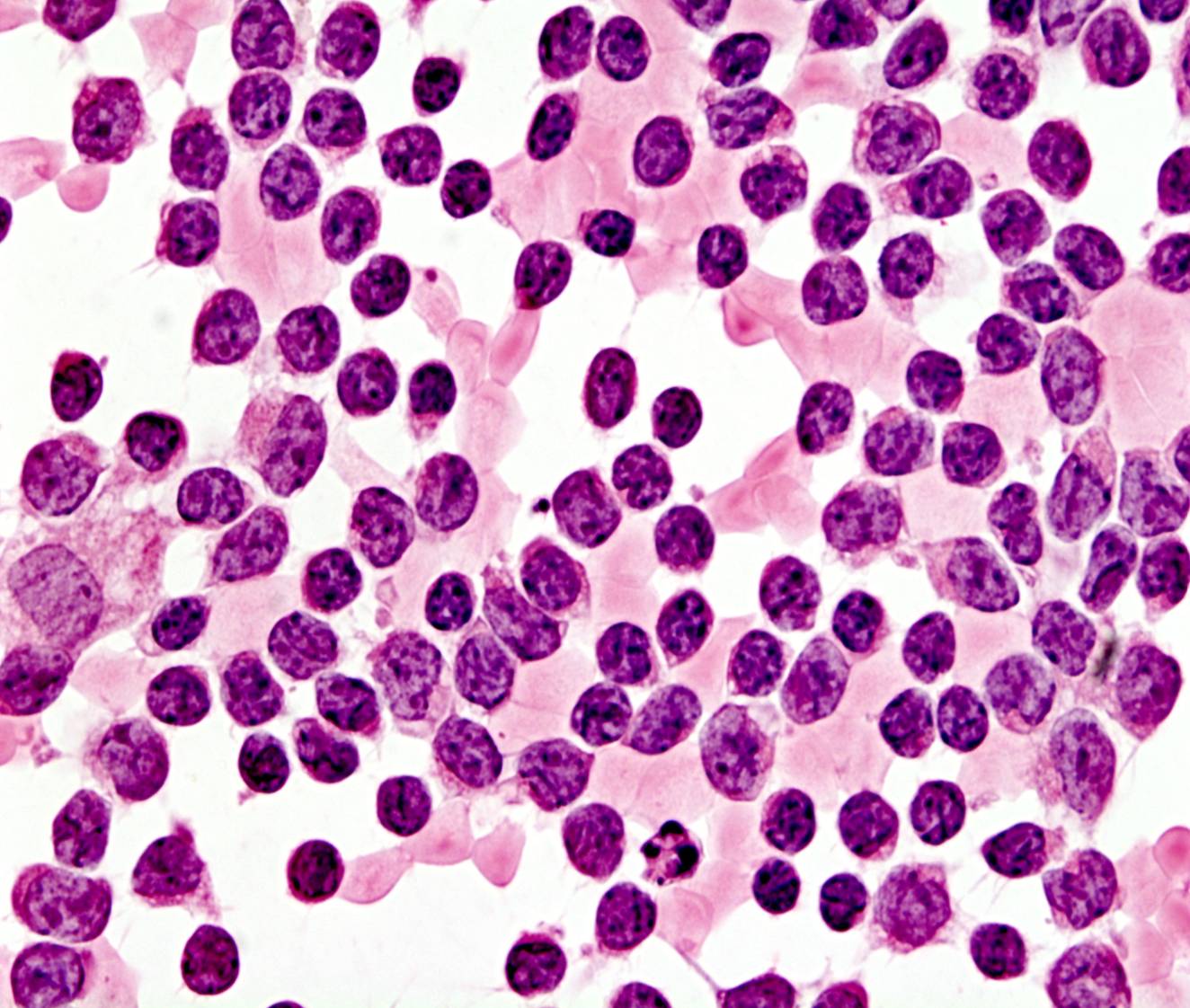
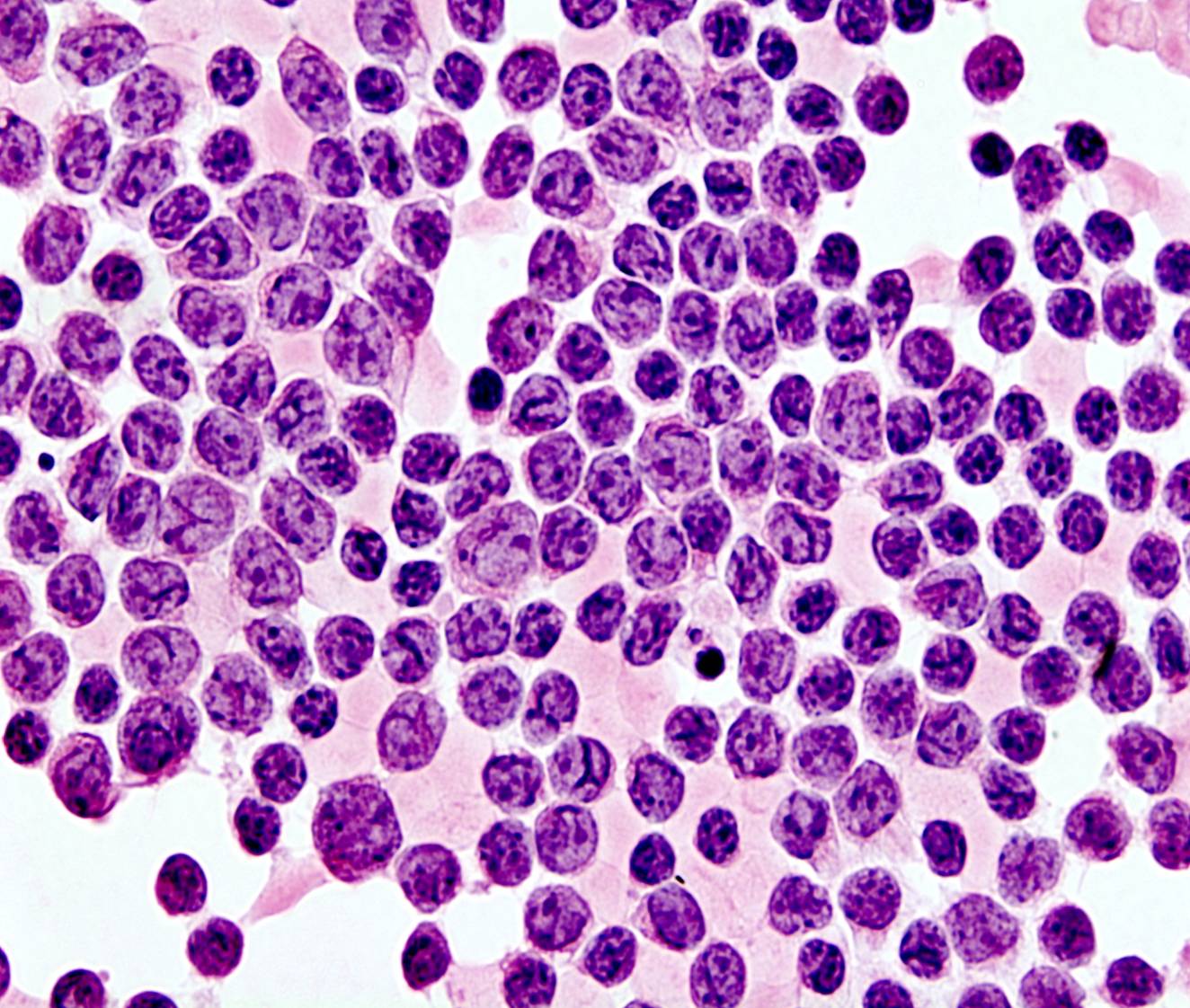
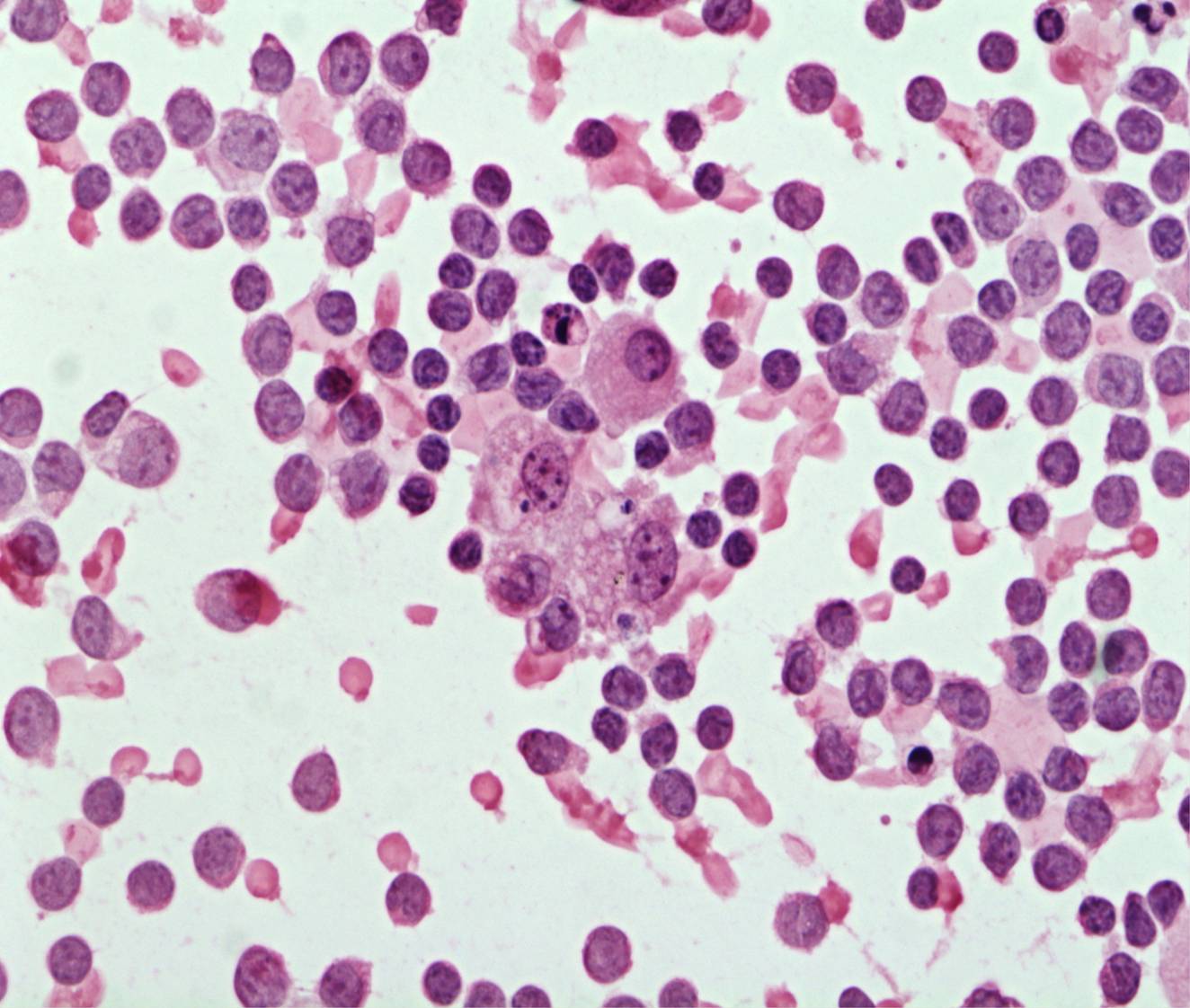
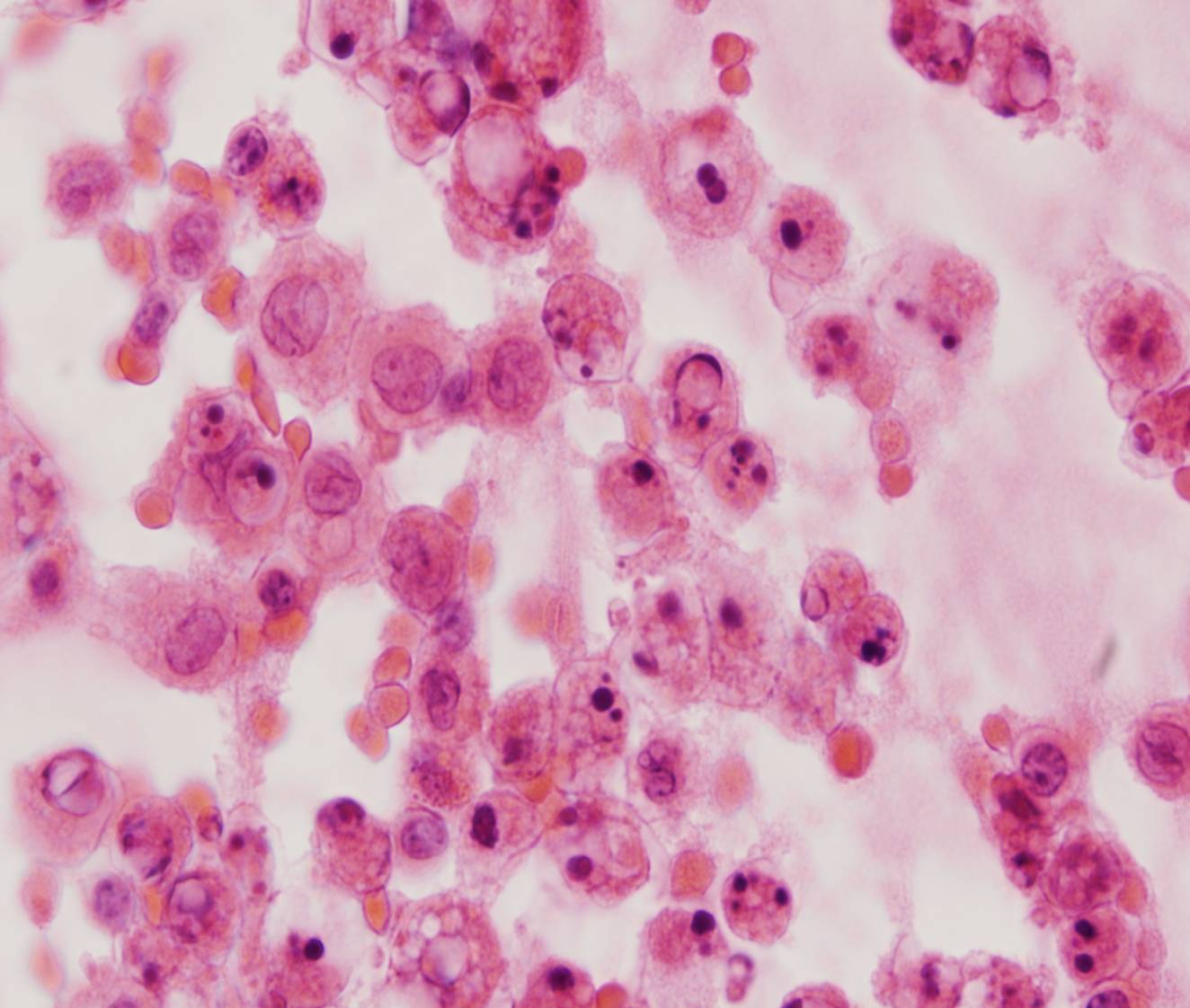
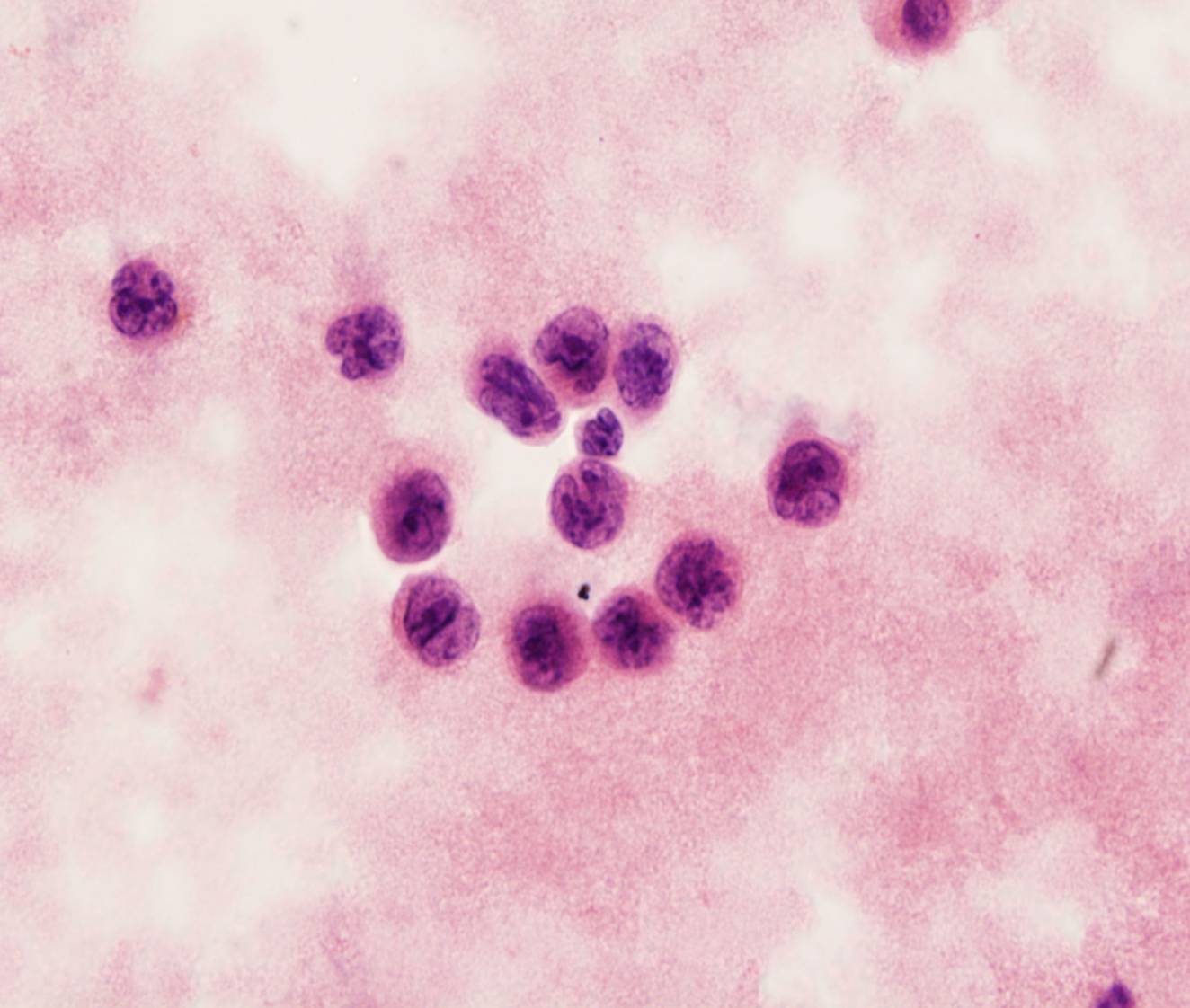
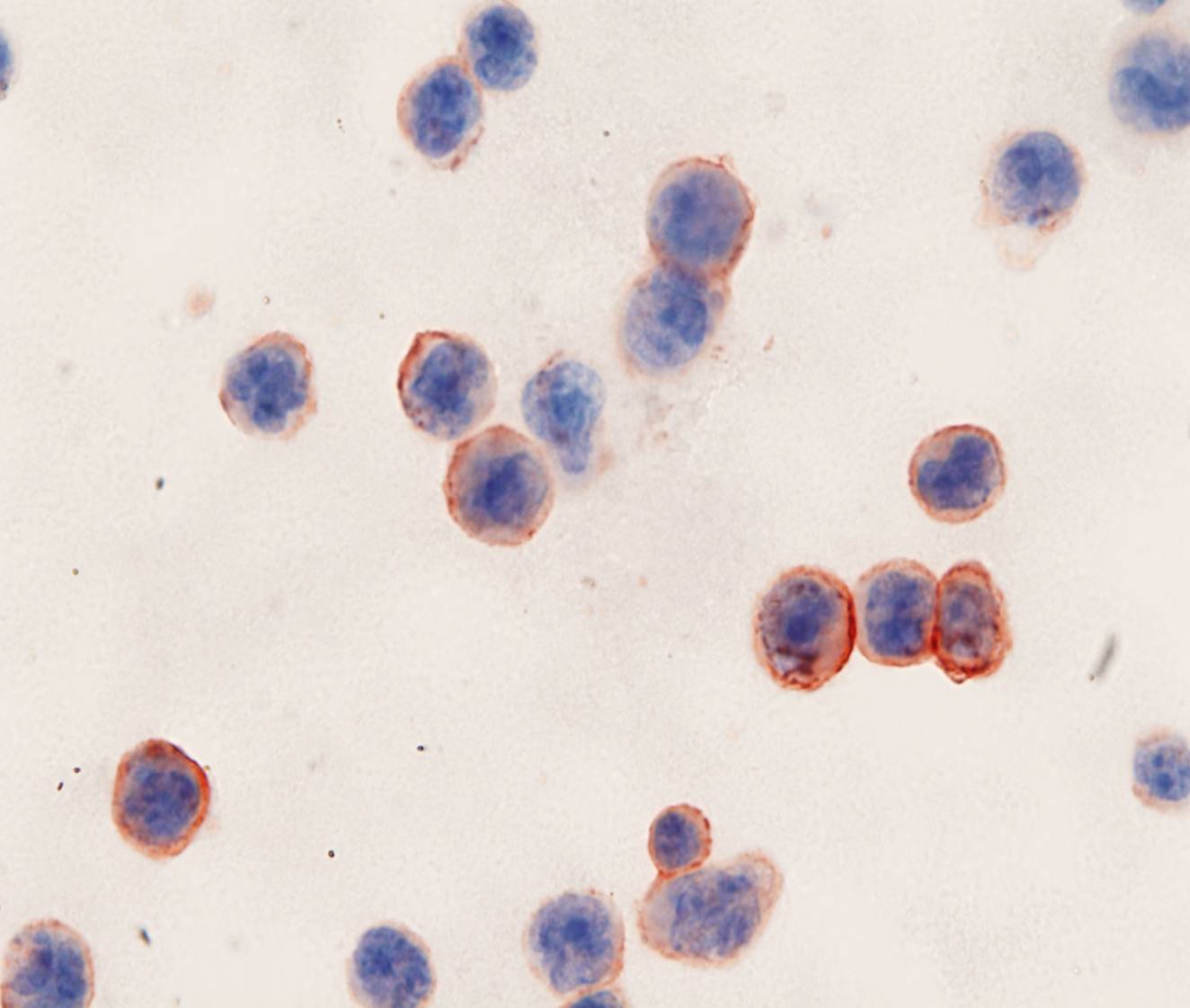
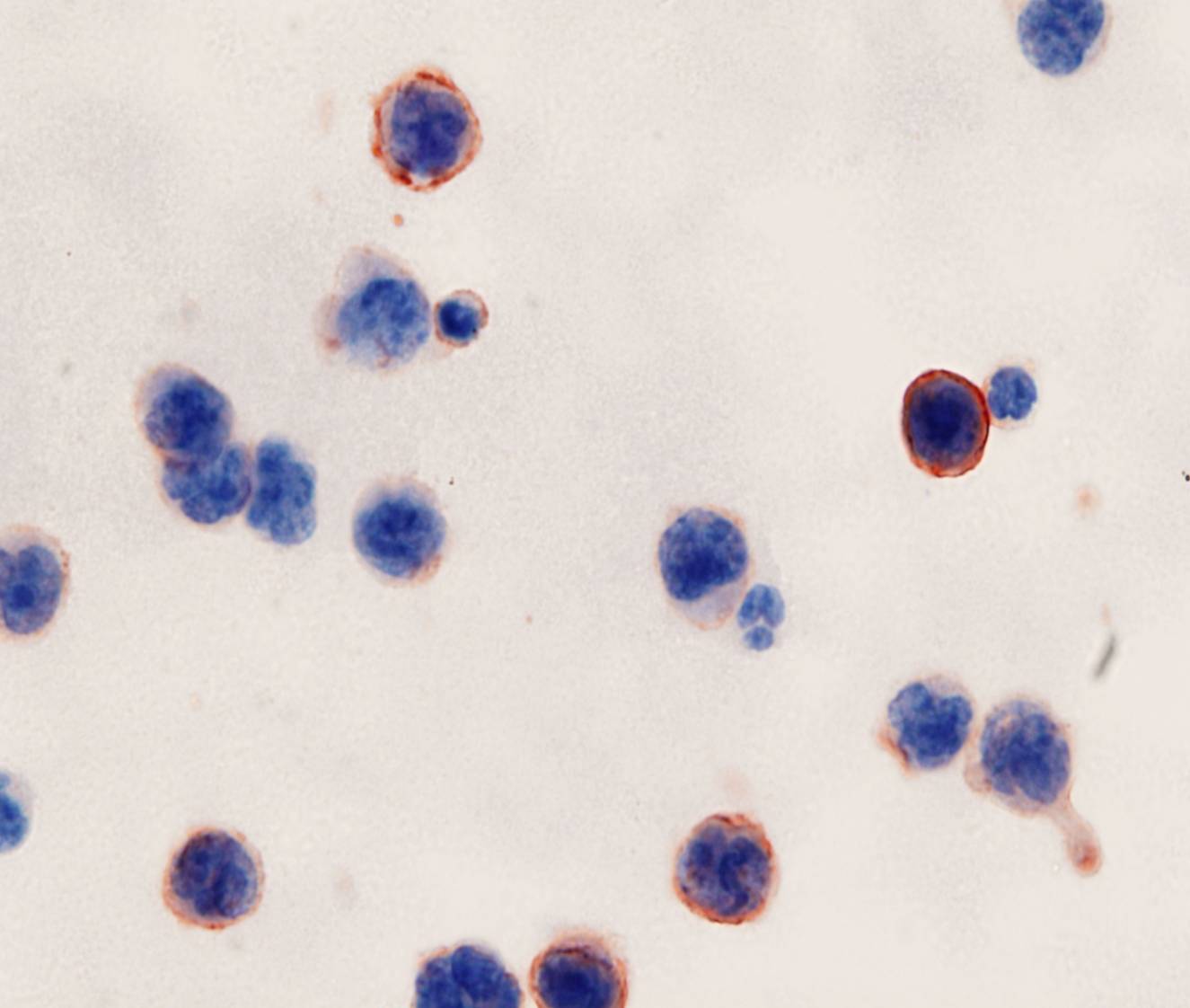
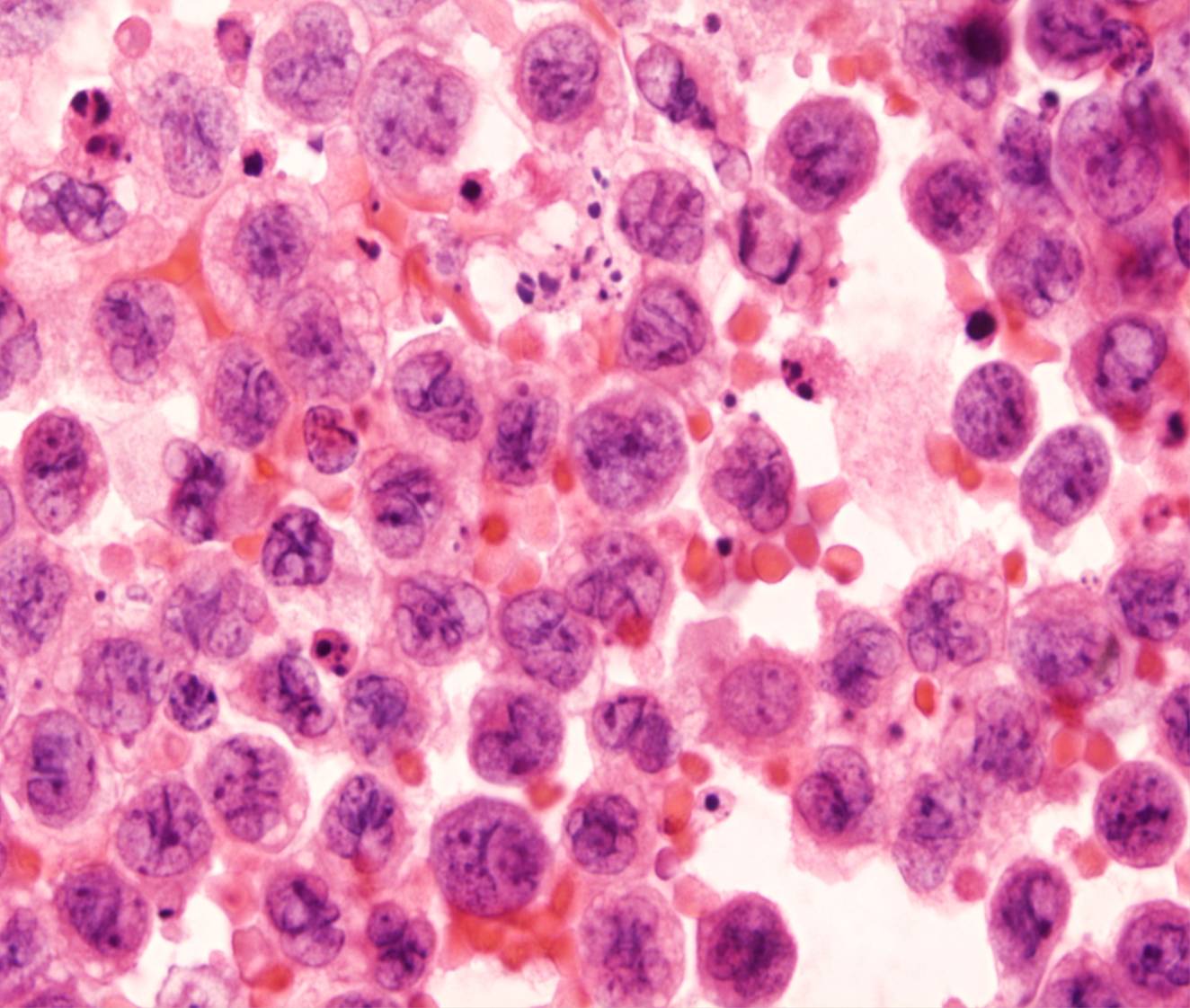
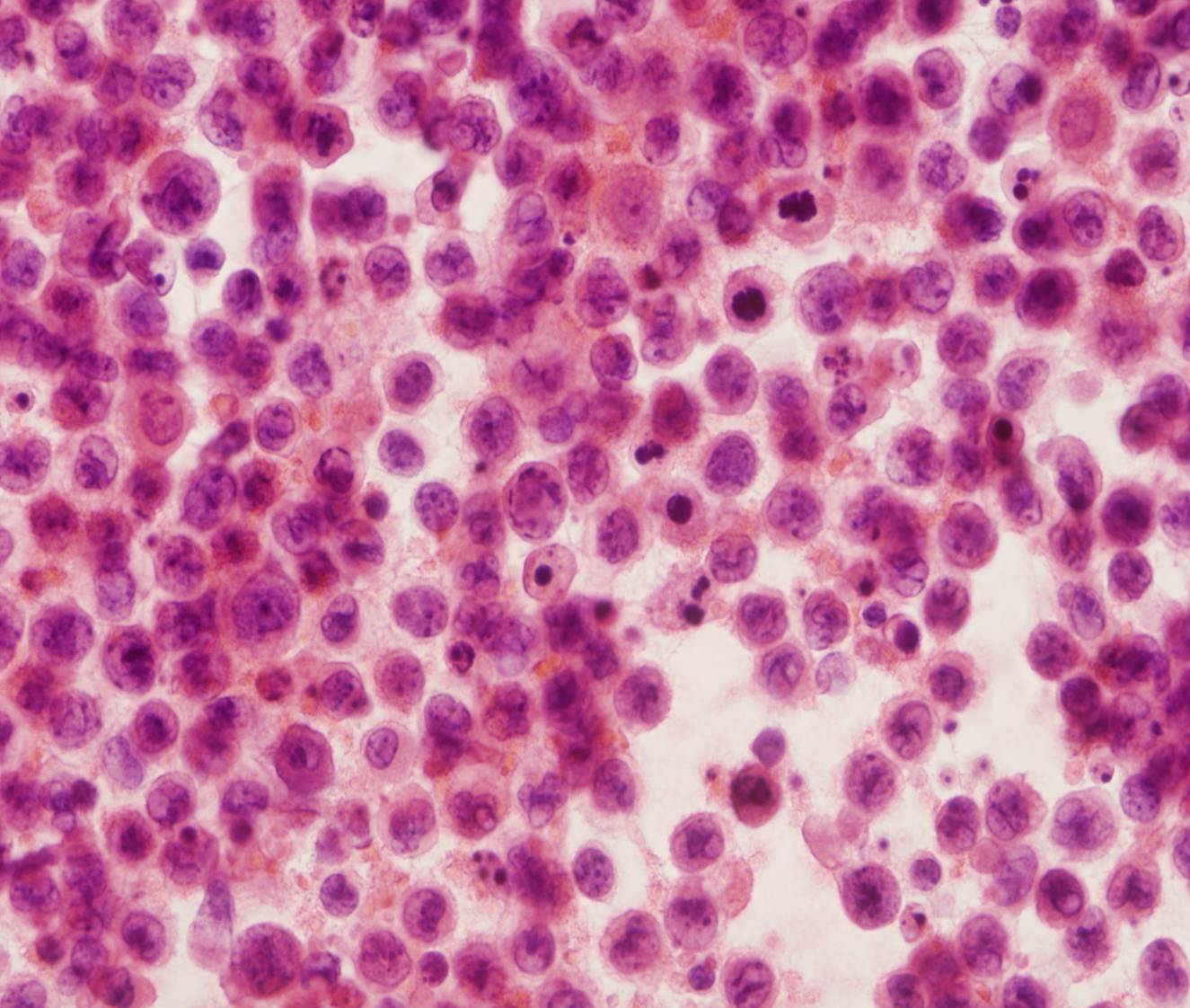
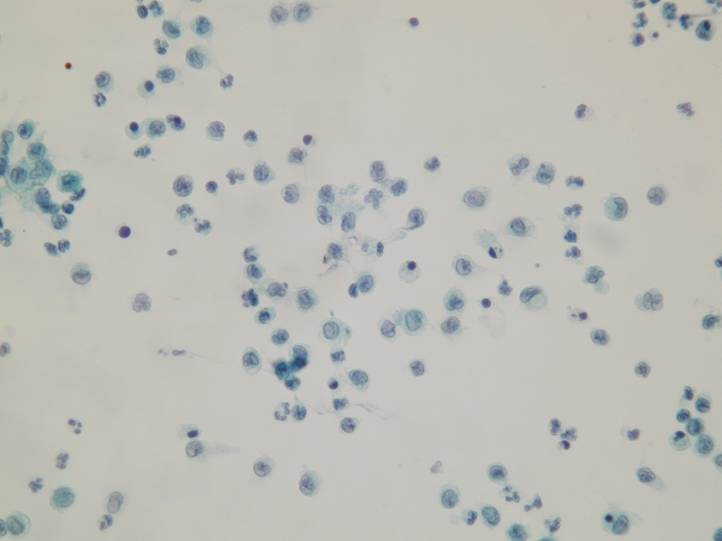
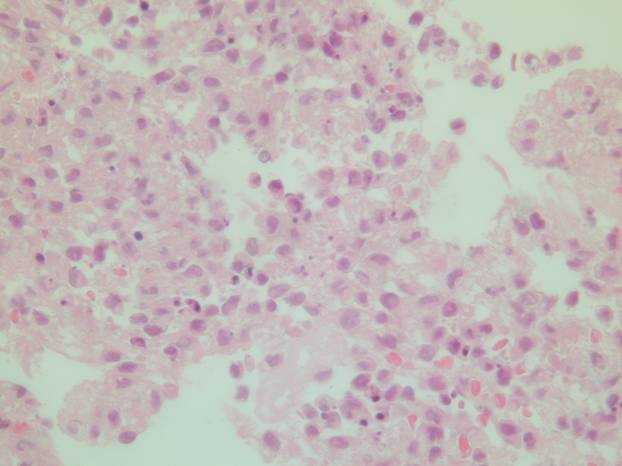
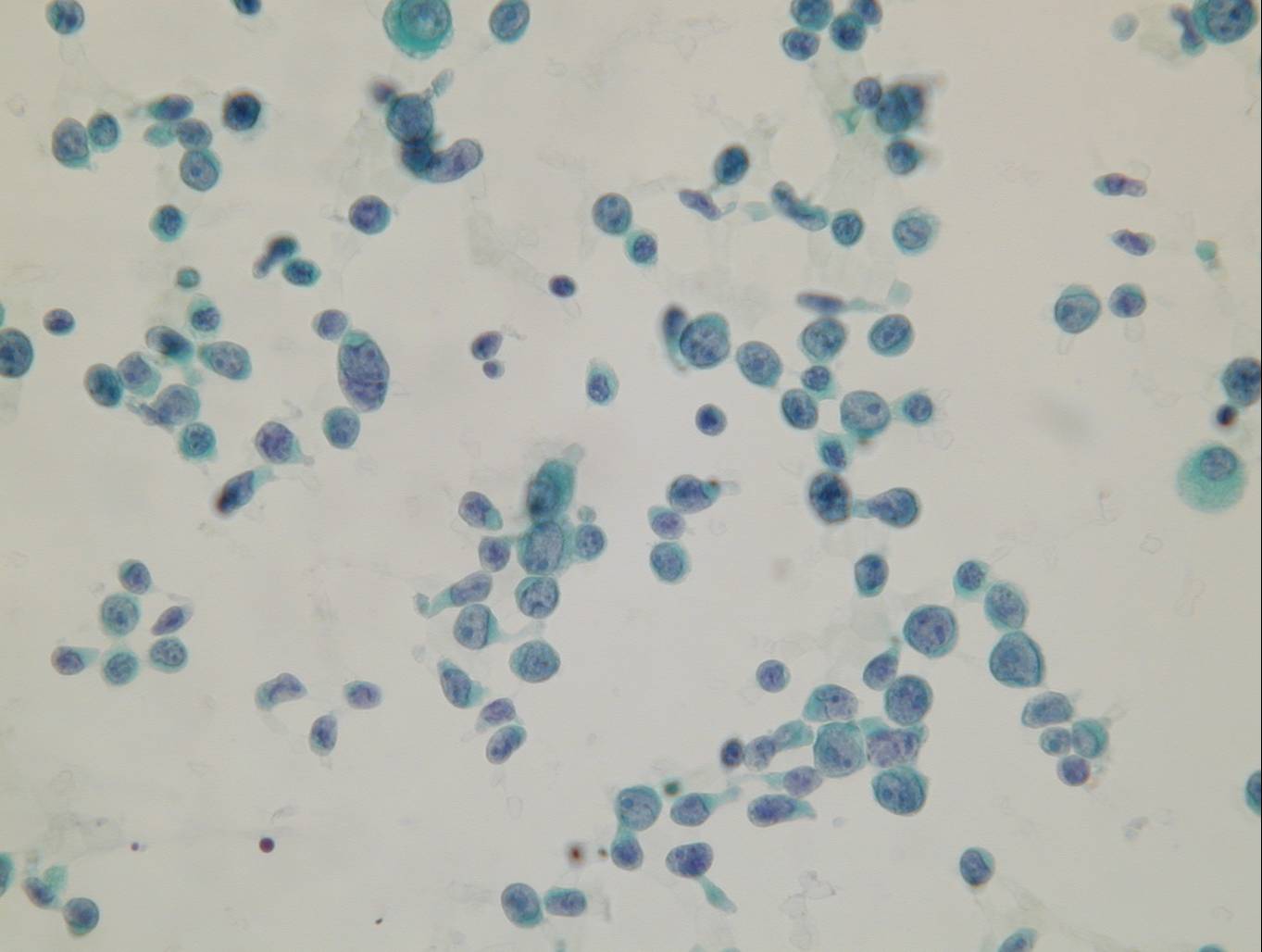
A malignant effusion may appear in the course of disease in many patients with non-Hodgkin lymphoma. Cytologic preparations are highly cellular and composed of dispersed lymphoid cells. Mesothelial cells may be absent.
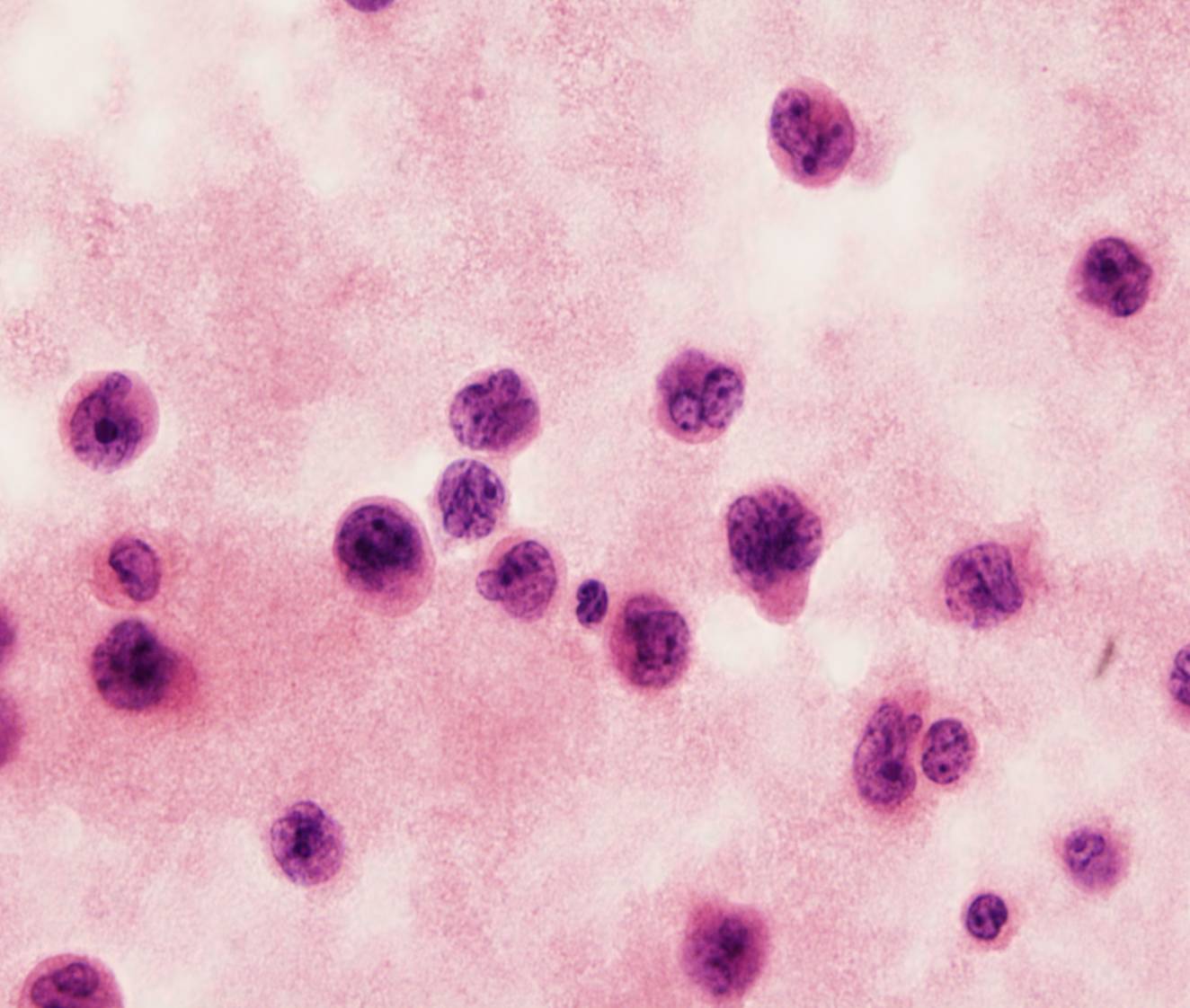
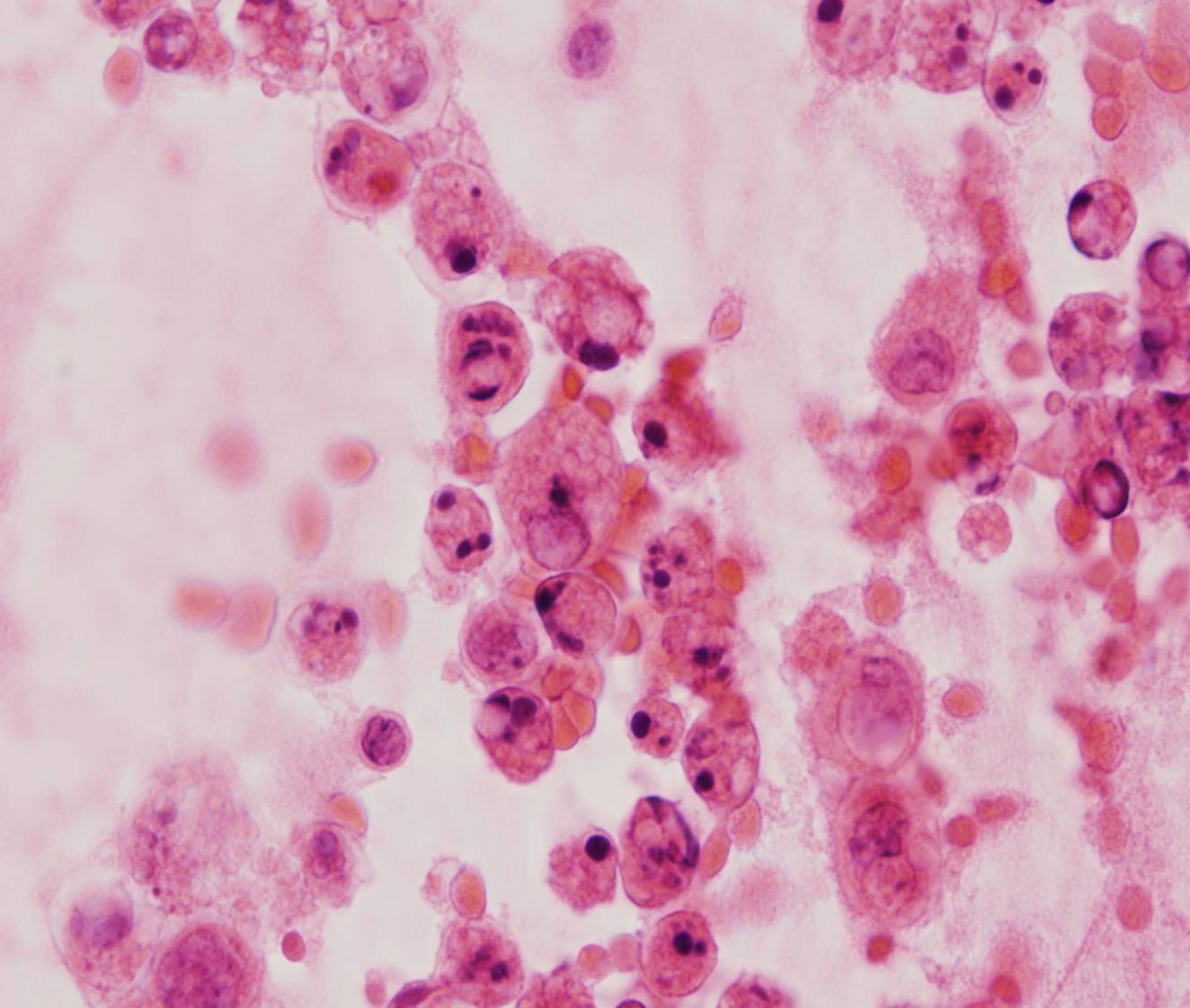
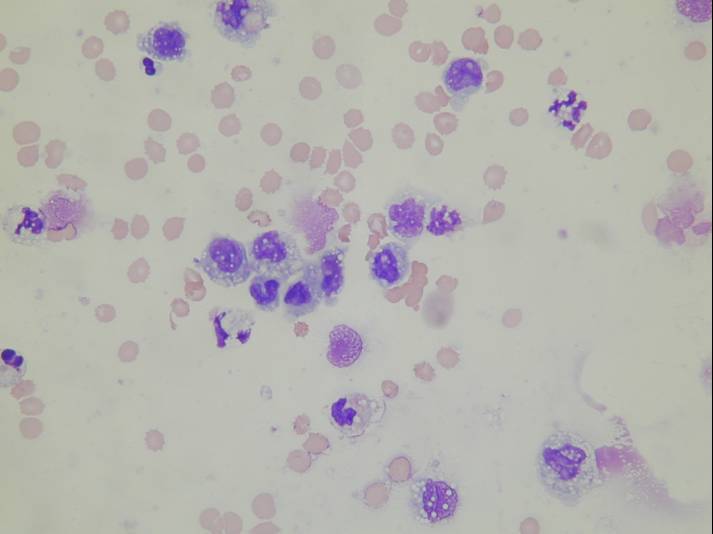
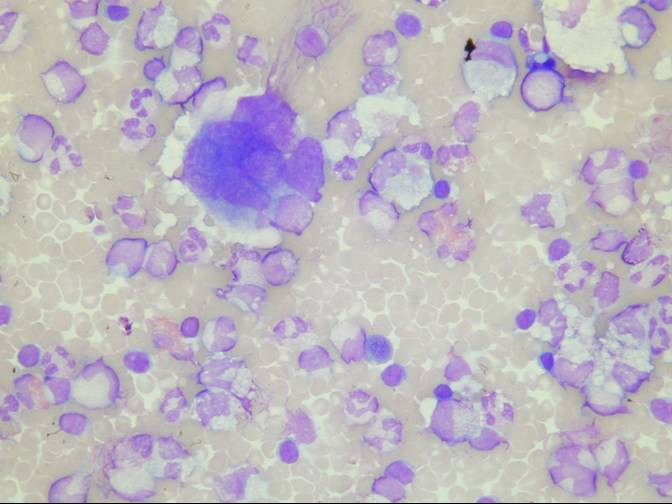
Several histologic types of non-Hodgkin lymphoma may involve the serosal cavities. The cells of large B-cell lymphomas have abundant, pale and vacuolated cytoplasm, and round or irregular nuclei with coarse chromatin. The cells of small cell lymphomas are only slightly larger than lymphocytes. Also follicular lymphomas, lymphoblastic lymphoma and Burkitt lymphoma can involve the serosal cavities. Karyorrhexis is a conspicuous feature of many lymphomas.
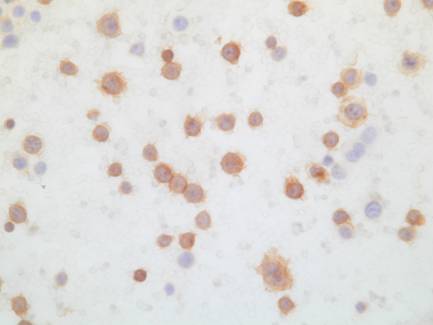
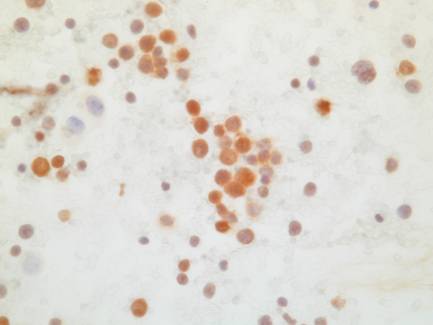
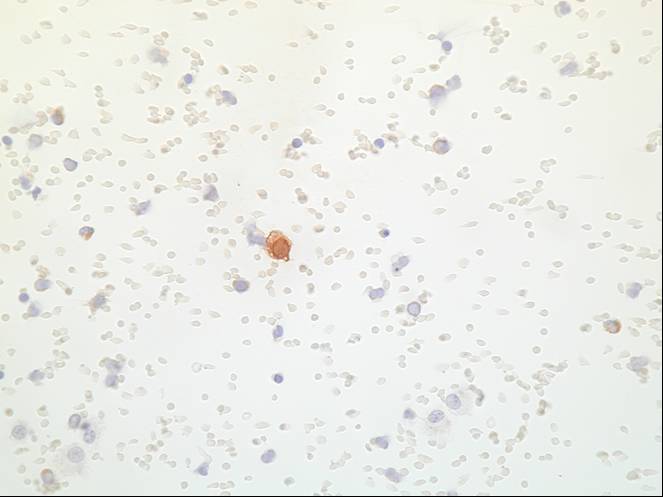
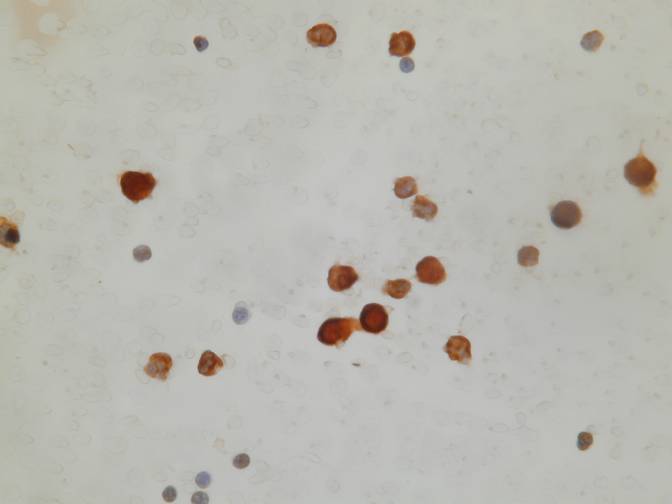
The differential diagnosis of small cell lymphomas includes benign effusions such as those due to tuberculosis, in which the fluid is composed predominantly of mature lymphocytes. The cells of small cell lymphomas may be impossible to distinguish from mature lymphocytes with Papanicolaou stains, whereas in Romanowsky-stained preparations they have a prominent coarse chromatin clumping. In lymphocyte-rich effusions which are cytologically equivocal for malignancy, kappa and lambda light chain expression can be examined by immunocytochemistry or flow cytometry, in order to document light chain restriction. Lymphomas are rarely confused with other malignancies because other tumors tend to form cell clusters in effusion. If there is any doubt about the lymphoid nature of malignant cells, an immunocytochemical panel of antibodies can be performed.
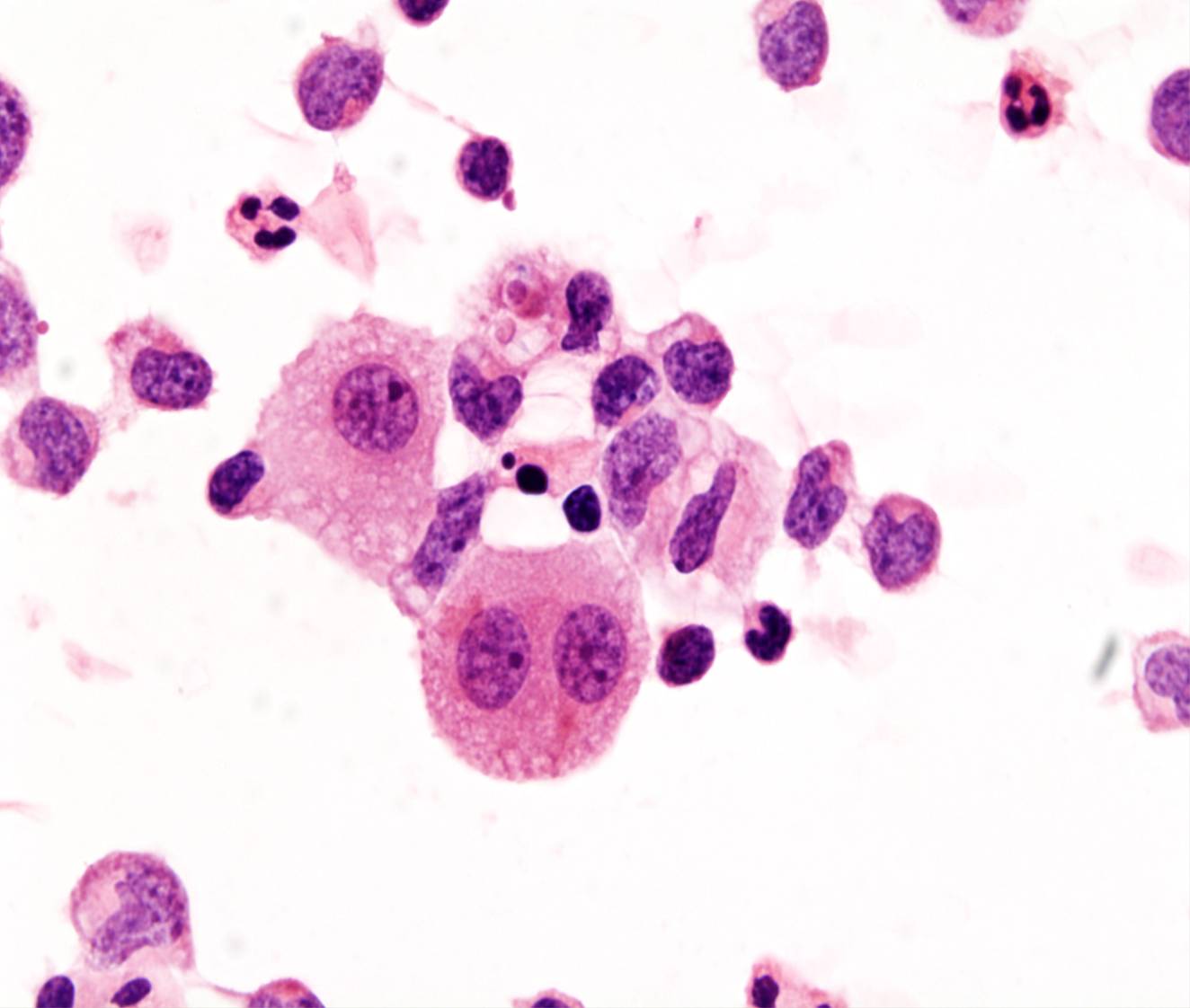
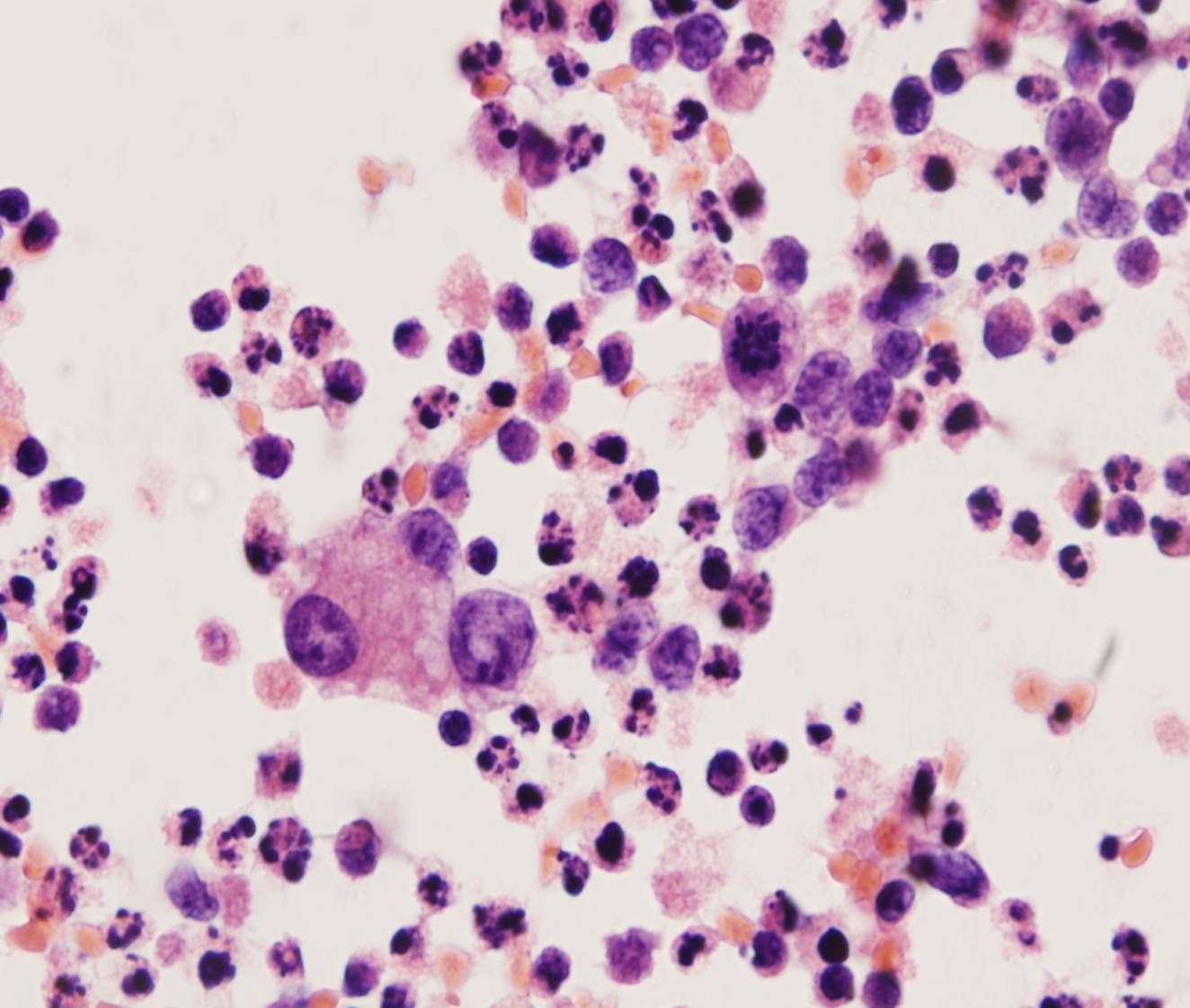
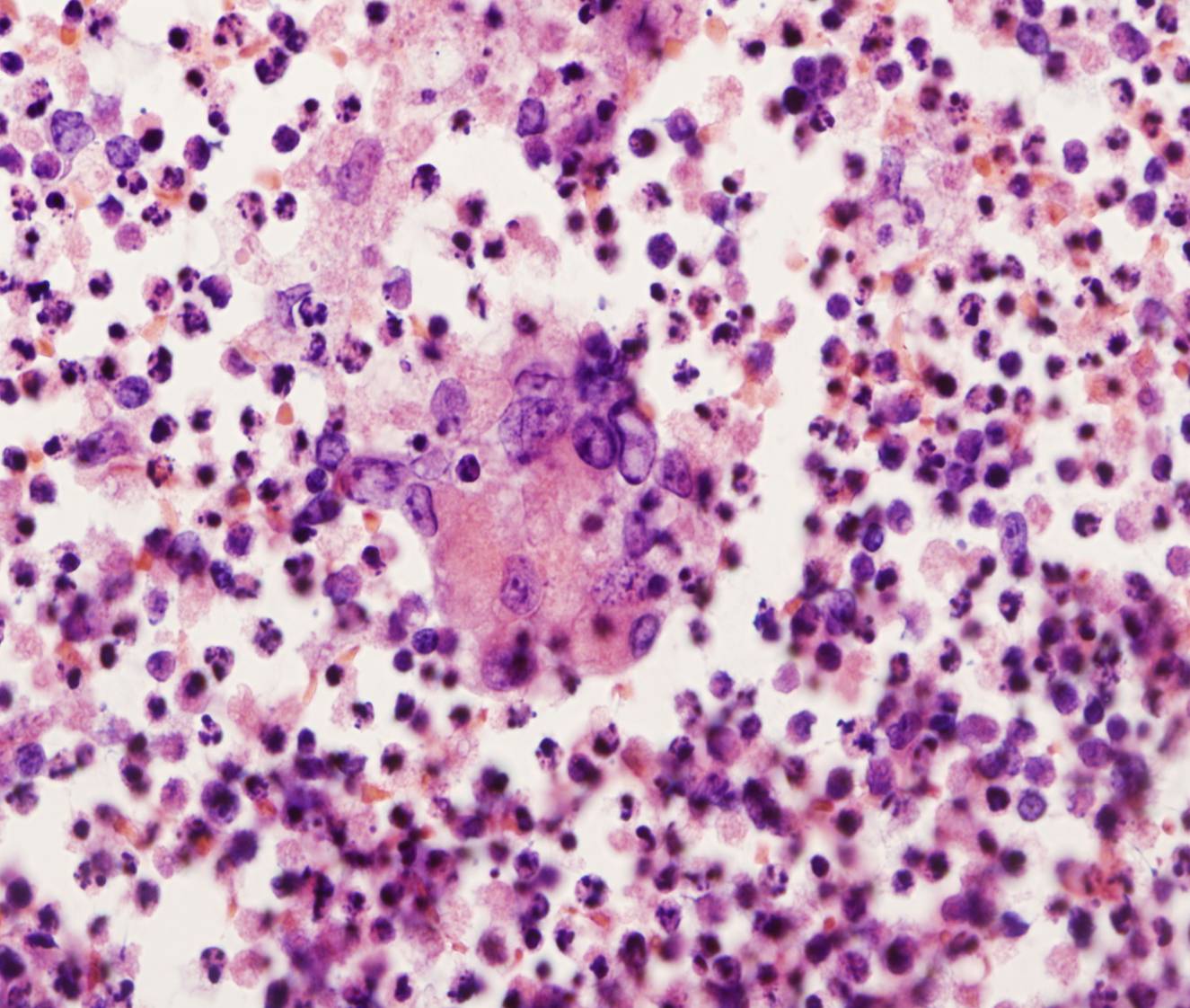
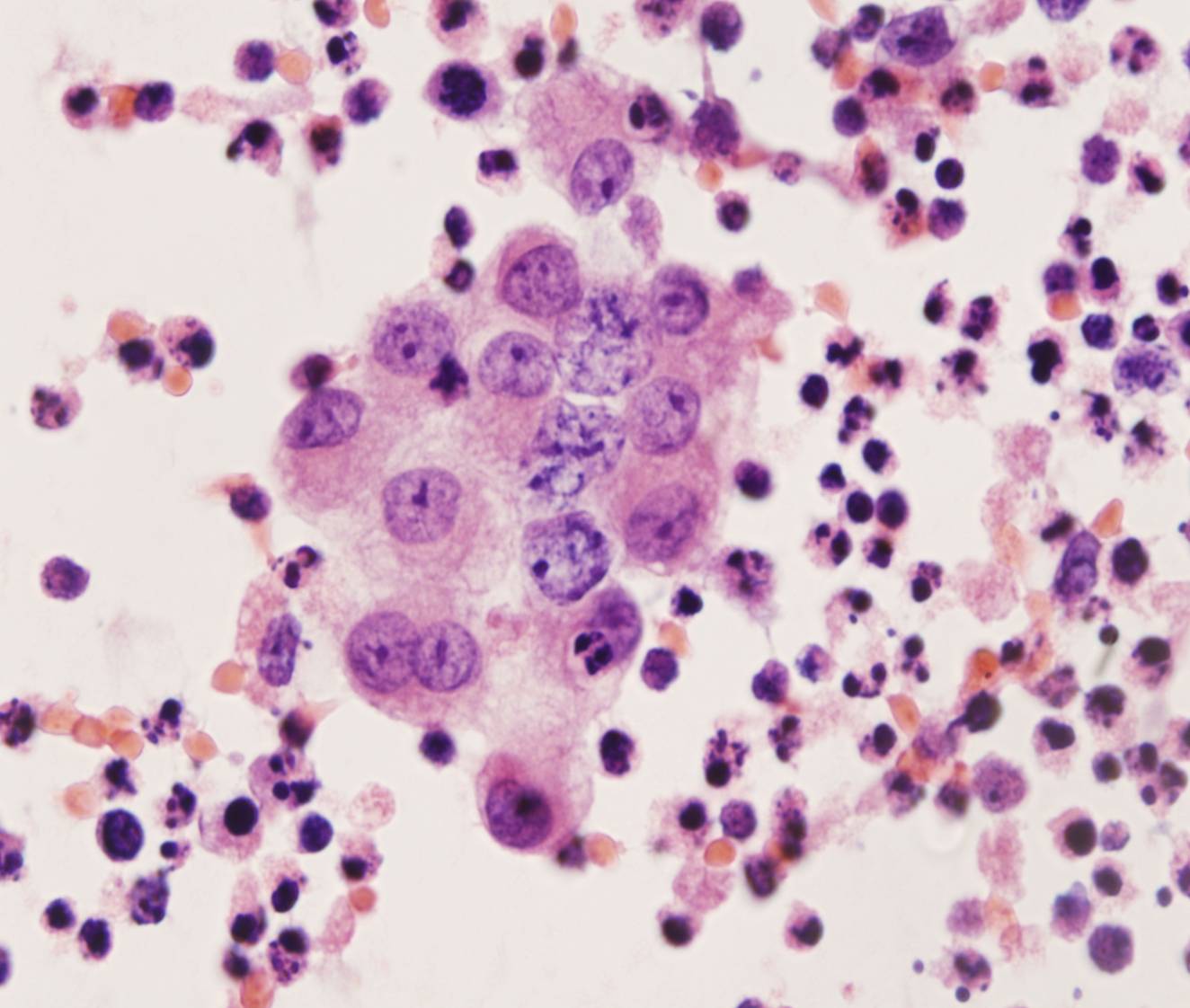
Malignant effusions are uncommon in Hodgkin lymphoma. The cytologic hallmark is the Reed-Sternberg cell, a large multinucleated cell with huge inclusion-like nucleoli. Mononuclear variants are also present, together with a mixed population of inflammatory cells including lymphocytes, plasma cells, histiocytes, eosinophils and neutrophils.
Other hematopoetic malignancies may involve the serosal cavities, such as acute lymphoblastic and myeloblastic leukemias and chronic leukemias.
136 137 138 139 140
141 142 143 144 145 146
147 148 149 150 151 152
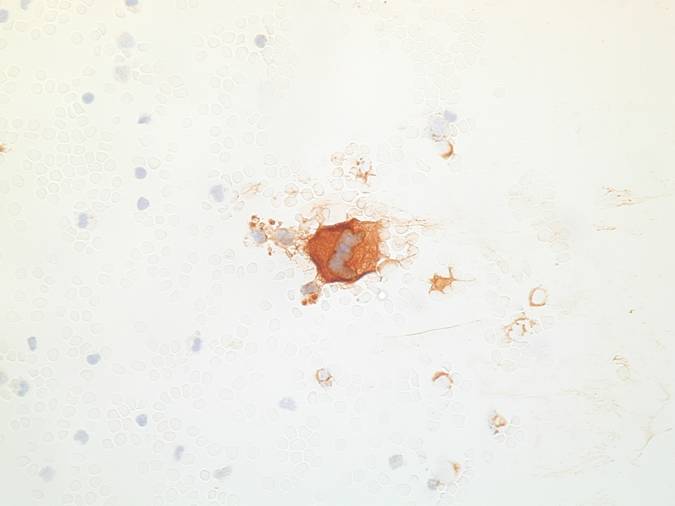
CML in myieloid blst crisis 156 CML in myieloid blst crisis - LCA157
Myelofibrosis159 ectopic myelopoiesis 160 ectopic myelopoiesis - calretinin 161 ectopic myelopoiesis - Mpx 162 ectopic myelopoiesis - PGP3 163